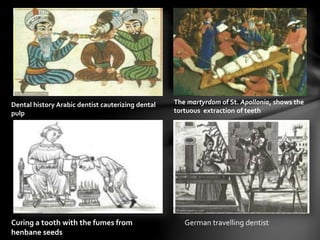
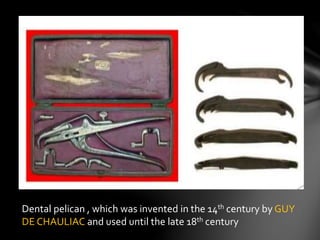
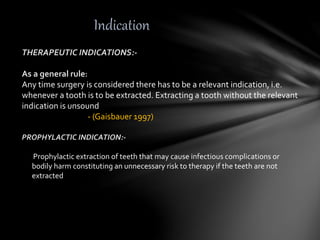
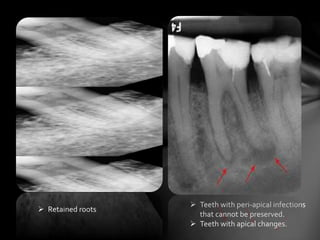
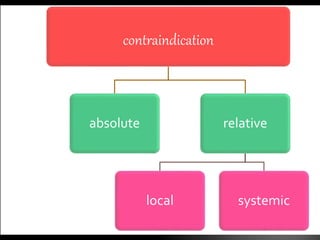
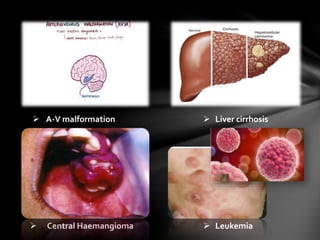
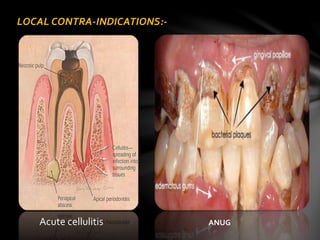
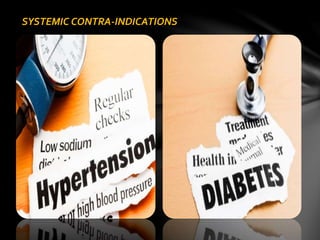
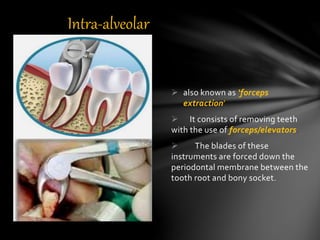
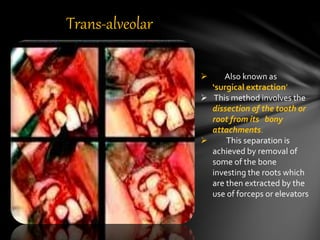
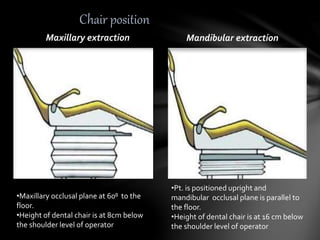
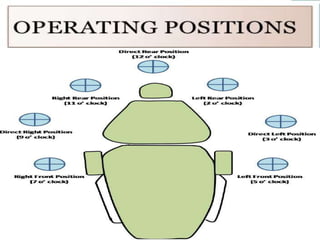
The document provides a comprehensive overview of exodontia, including its definition, historical context, and methods of tooth extraction. It details various indications and contraindications for extraction, as well as techniques and principles involved in the procedure. Additionally, it discusses post-operative instructions and potential complications associated with tooth extraction.