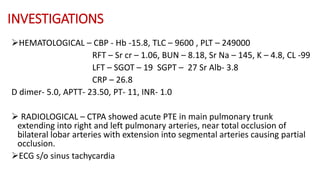
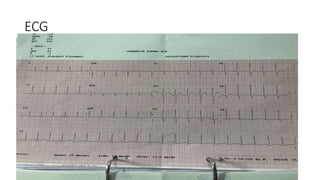
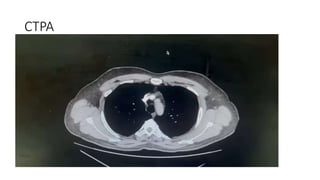
1) A 44-year-old male presented with shortness of breath and was found to have acute pulmonary embolism based on CTPA findings.
2) He underwent thrombolysis with tenecteplase but became unresponsive and required CPR, however CT brain was negative for hemorrhage.
3) The patient's condition deteriorated and he was started on vasopressors, mechanical thrombectomy was performed, and eventually venoarterial ECMO was initiated due to hemodynamic instability.