Downloaded 25 times
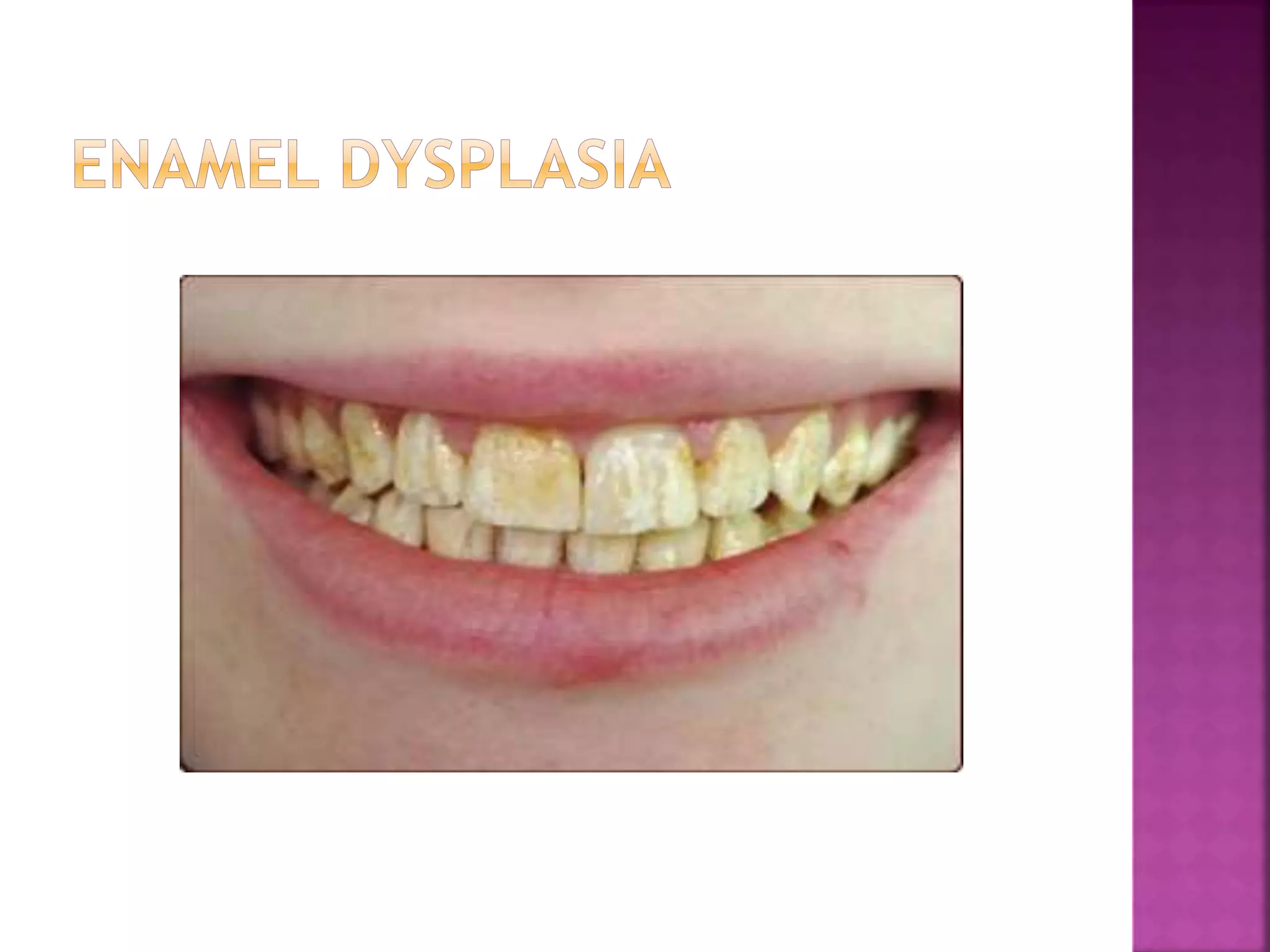
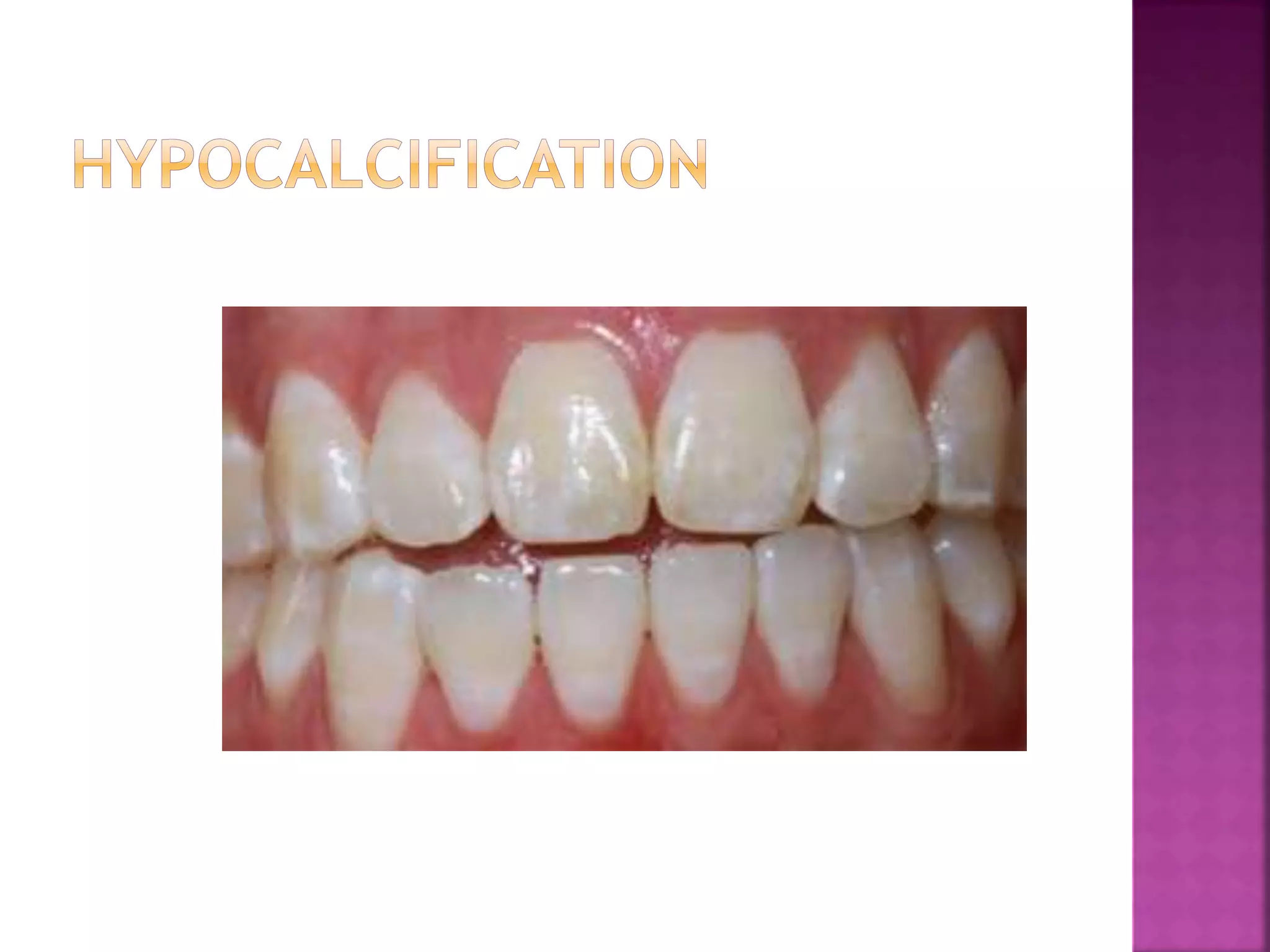
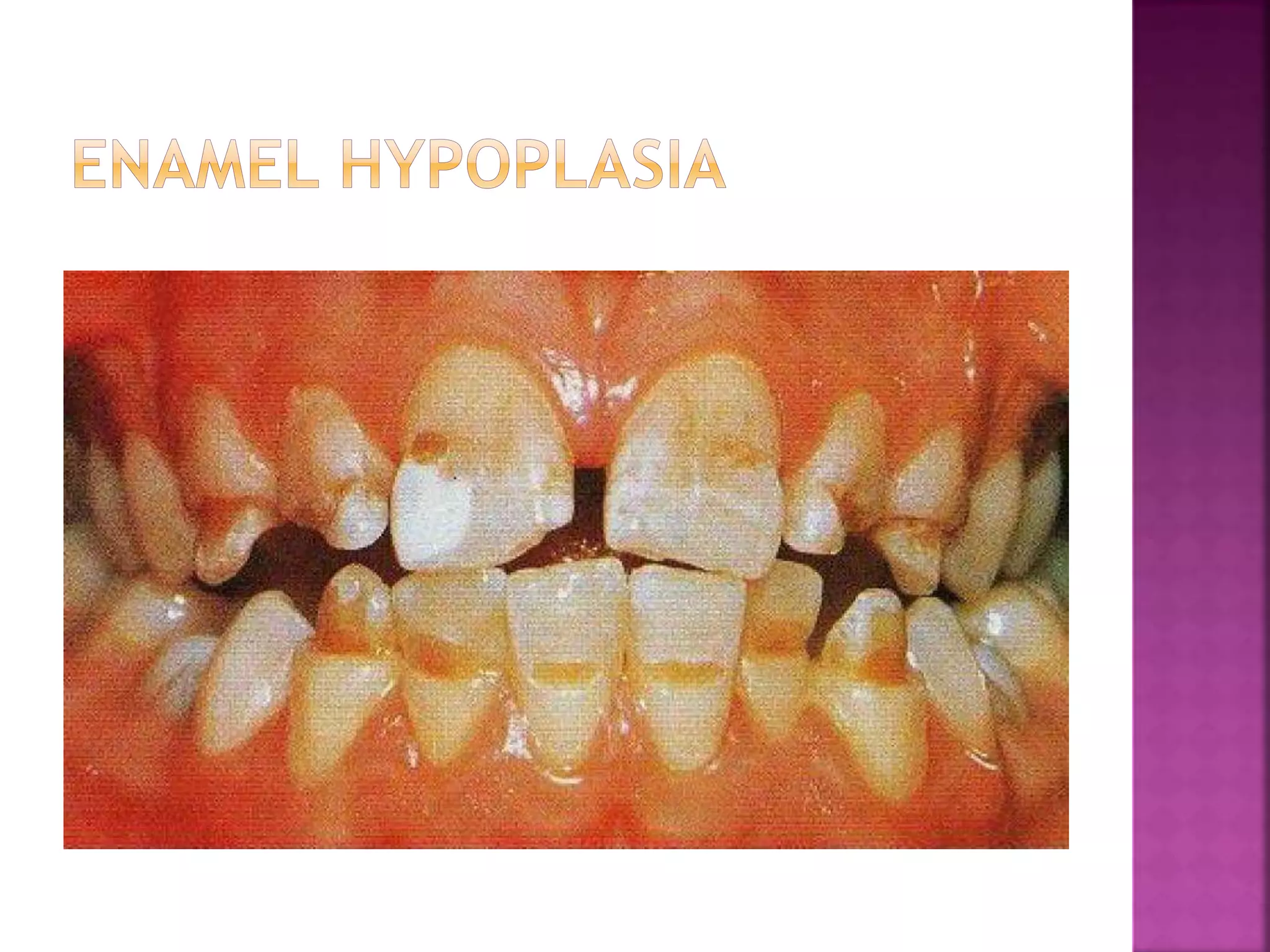
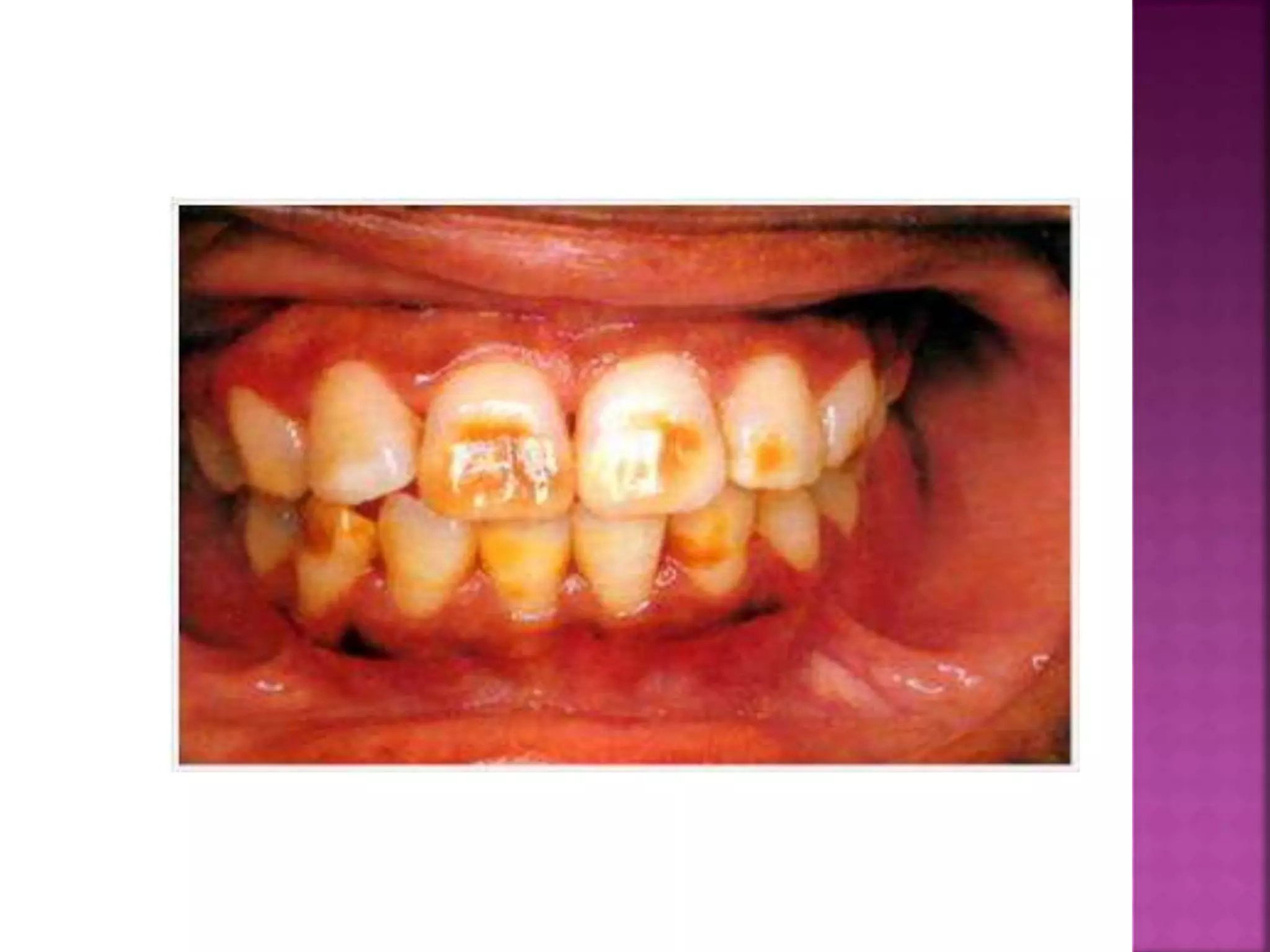


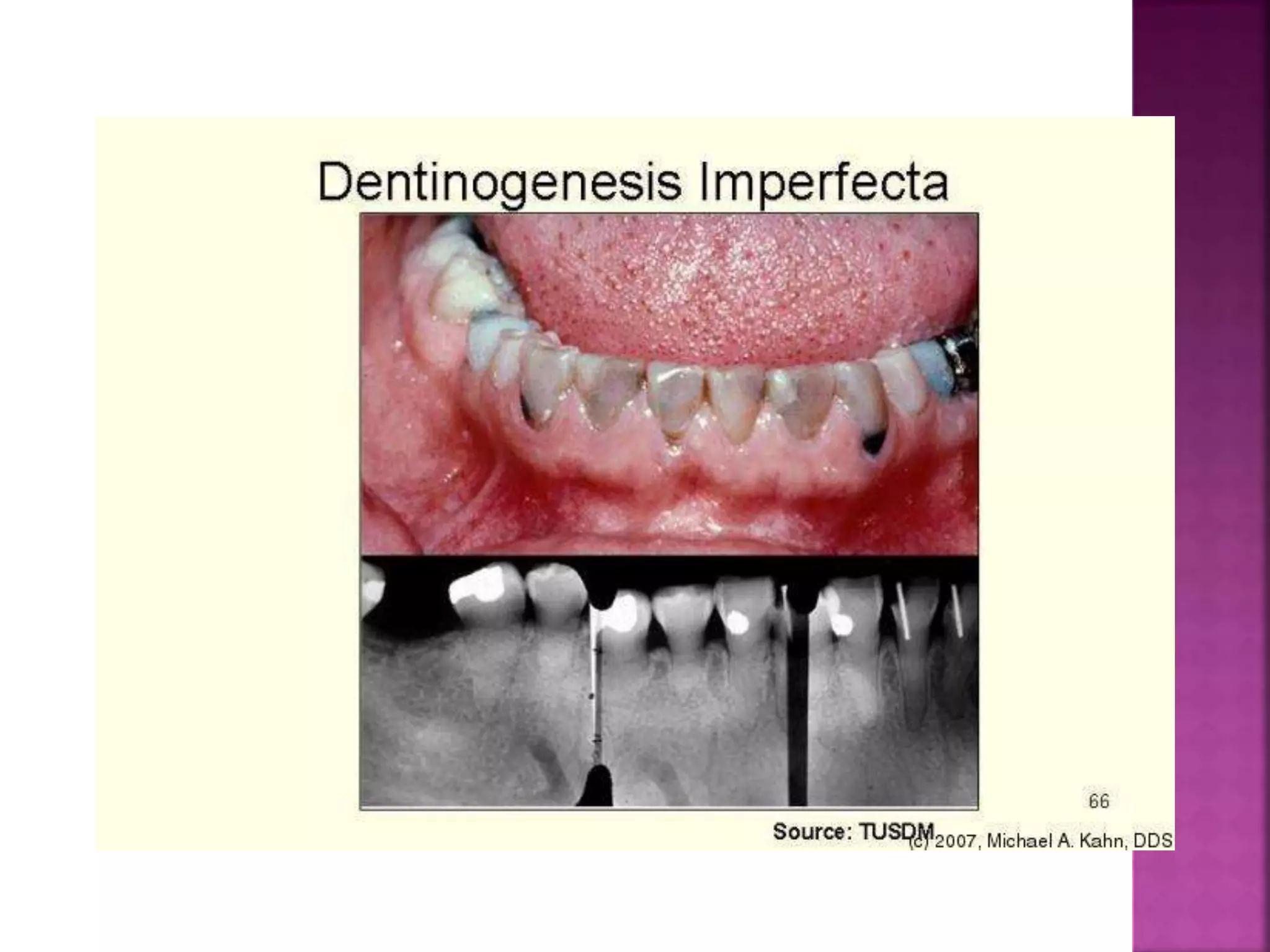

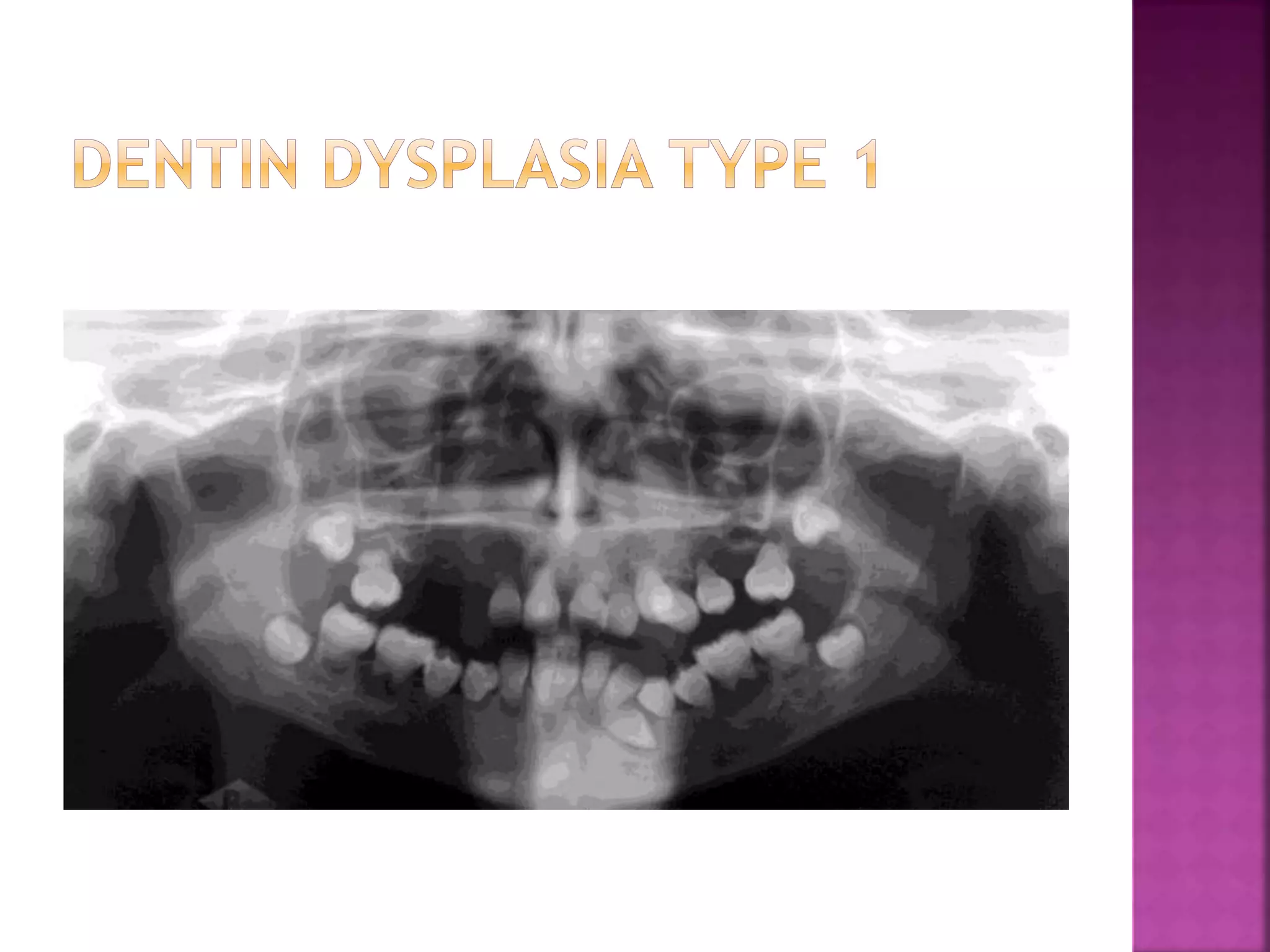
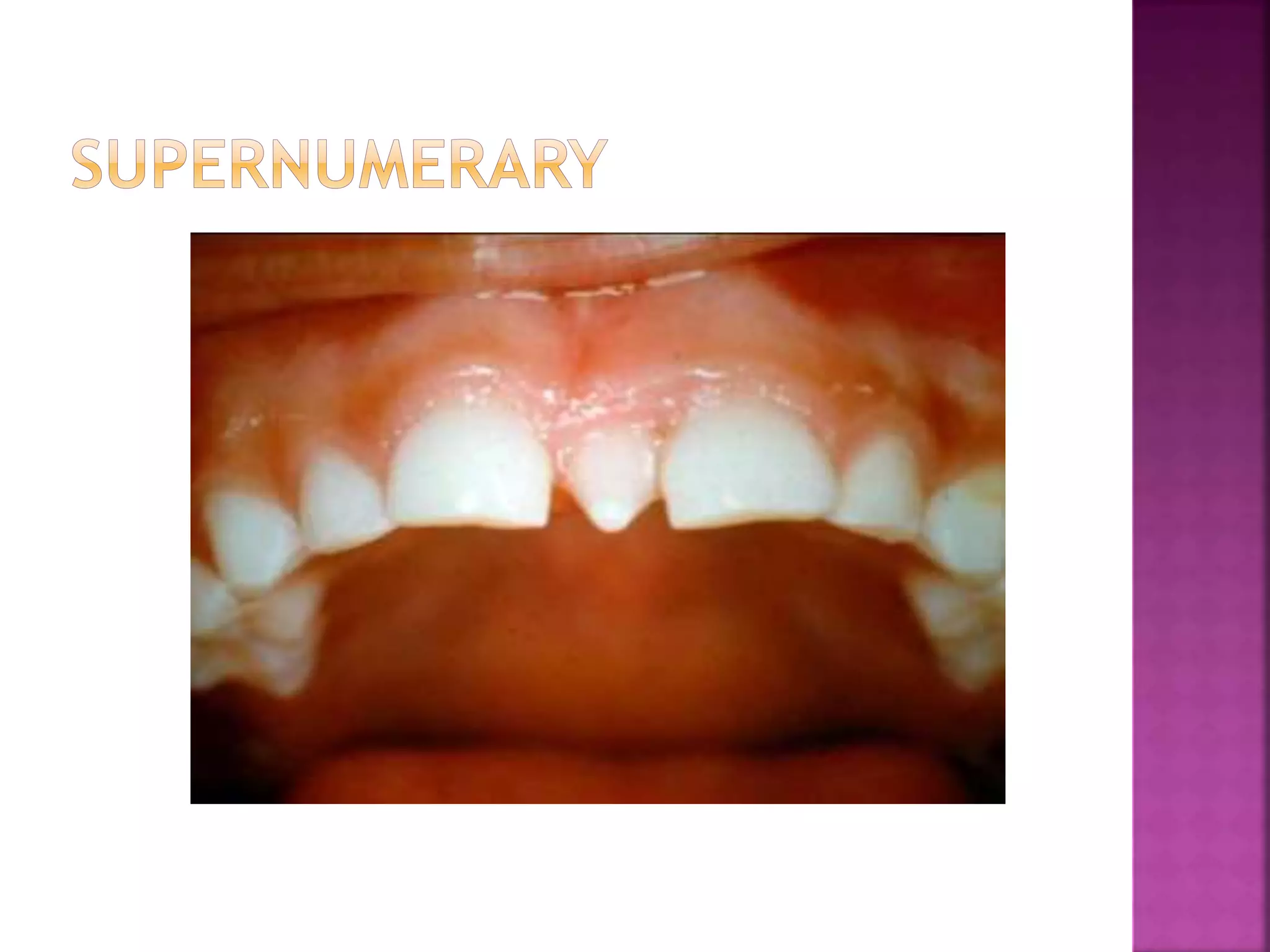




The document discusses various causes of tooth discoloration and abnormalities in tooth development and structure. It describes developmental disturbances that can result in discoloration, such as amelogenesis imperfecta or dental fluorosis. Intrinsic pigments from conditions like jaundice or blood disorders can also cause tooth discoloration. Abnormalities in tooth number, size, shape, structure, and enamel formation are discussed in relation to hereditary and environmental factors.





























































