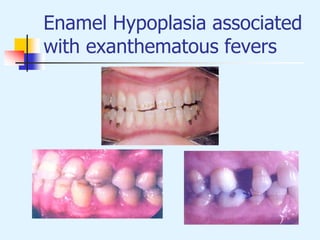
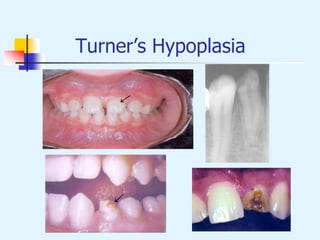
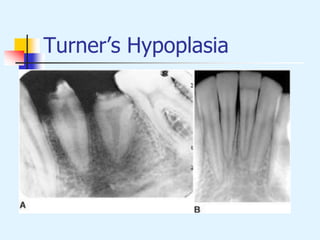
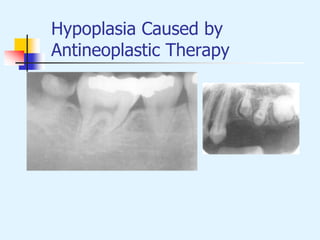
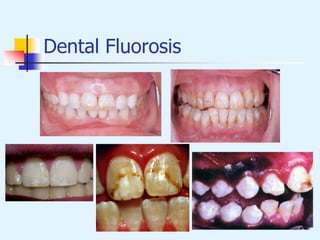
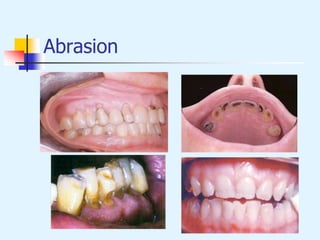
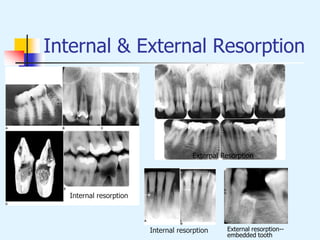
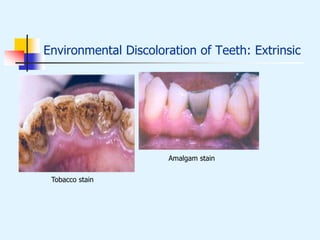
This document discusses various environmental effects that can cause abnormalities in tooth development and structure. It describes enamel hypoplasia, diffuse and demarcated opacities that can result from systemic influences like fevers during development. Turner's hypoplasia is discussed as being caused by trauma or inflammation from deciduous teeth. Other causes mentioned include antineoplastic therapy, dental fluorosis, syphilis, attrition, abrasion, erosion, and abfraction. Internal and external root resorption are also summarized, as well as extrinsic environmental discoloration of teeth from sources like staining, tobacco, and medications.