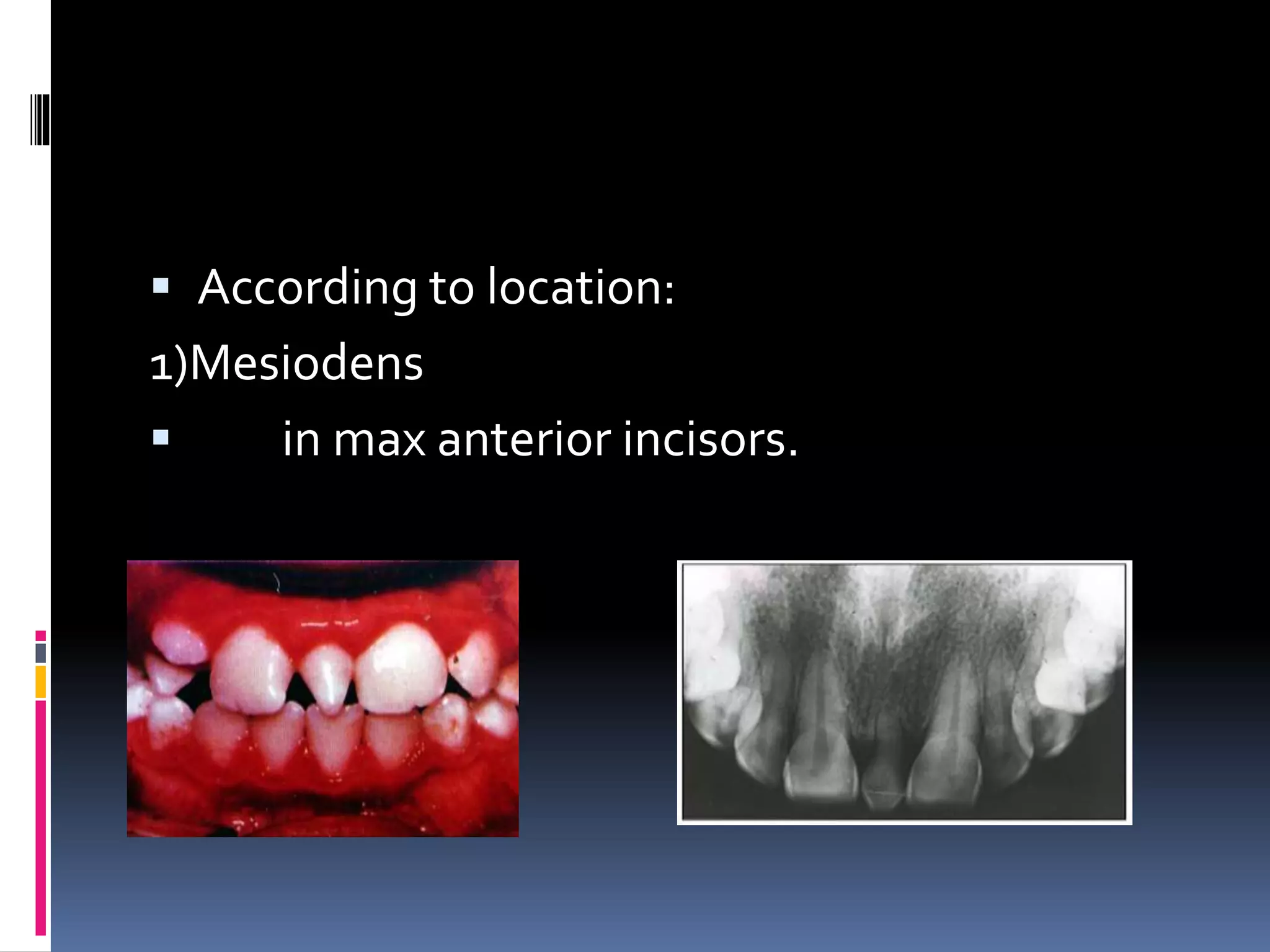
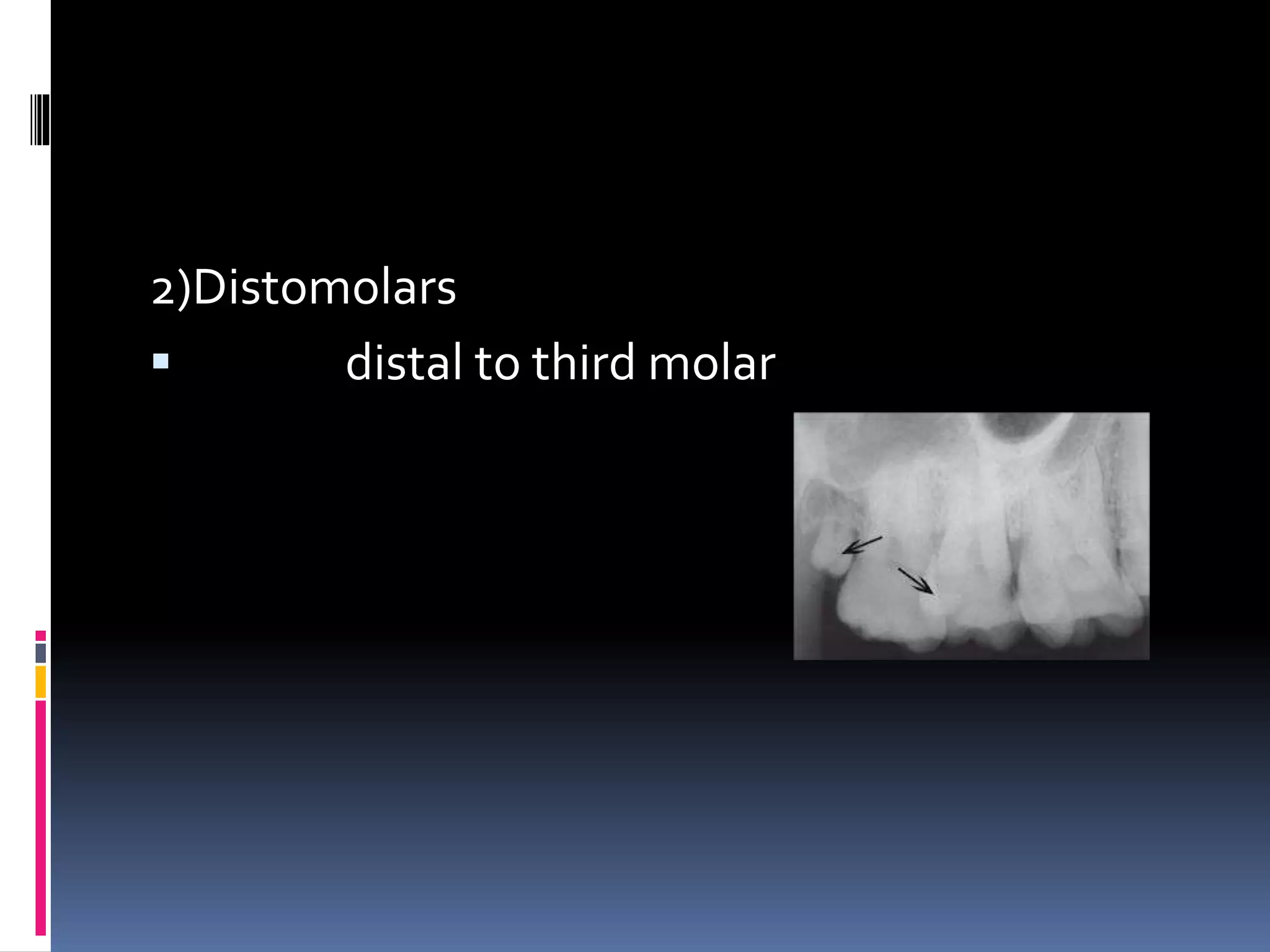
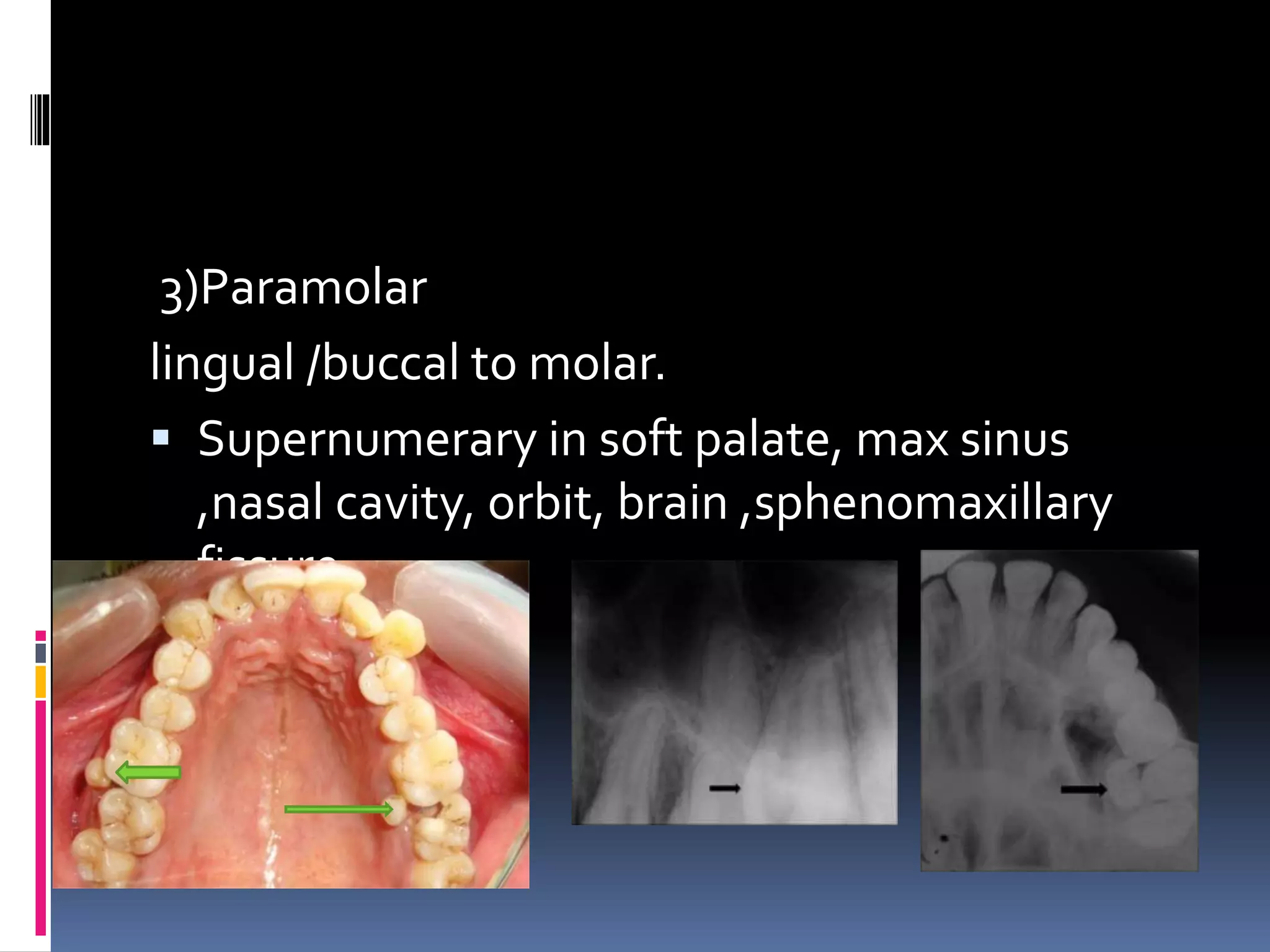
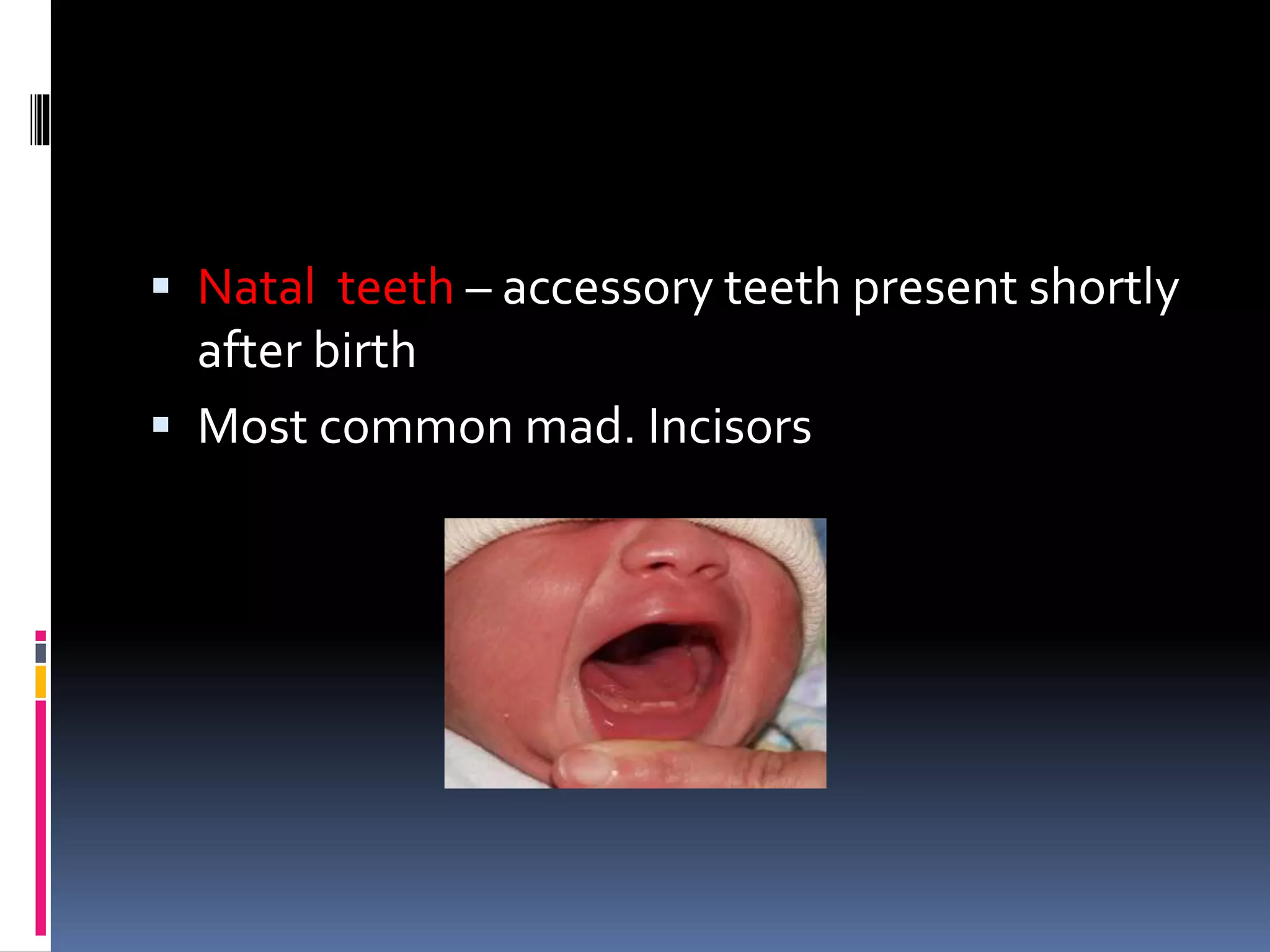
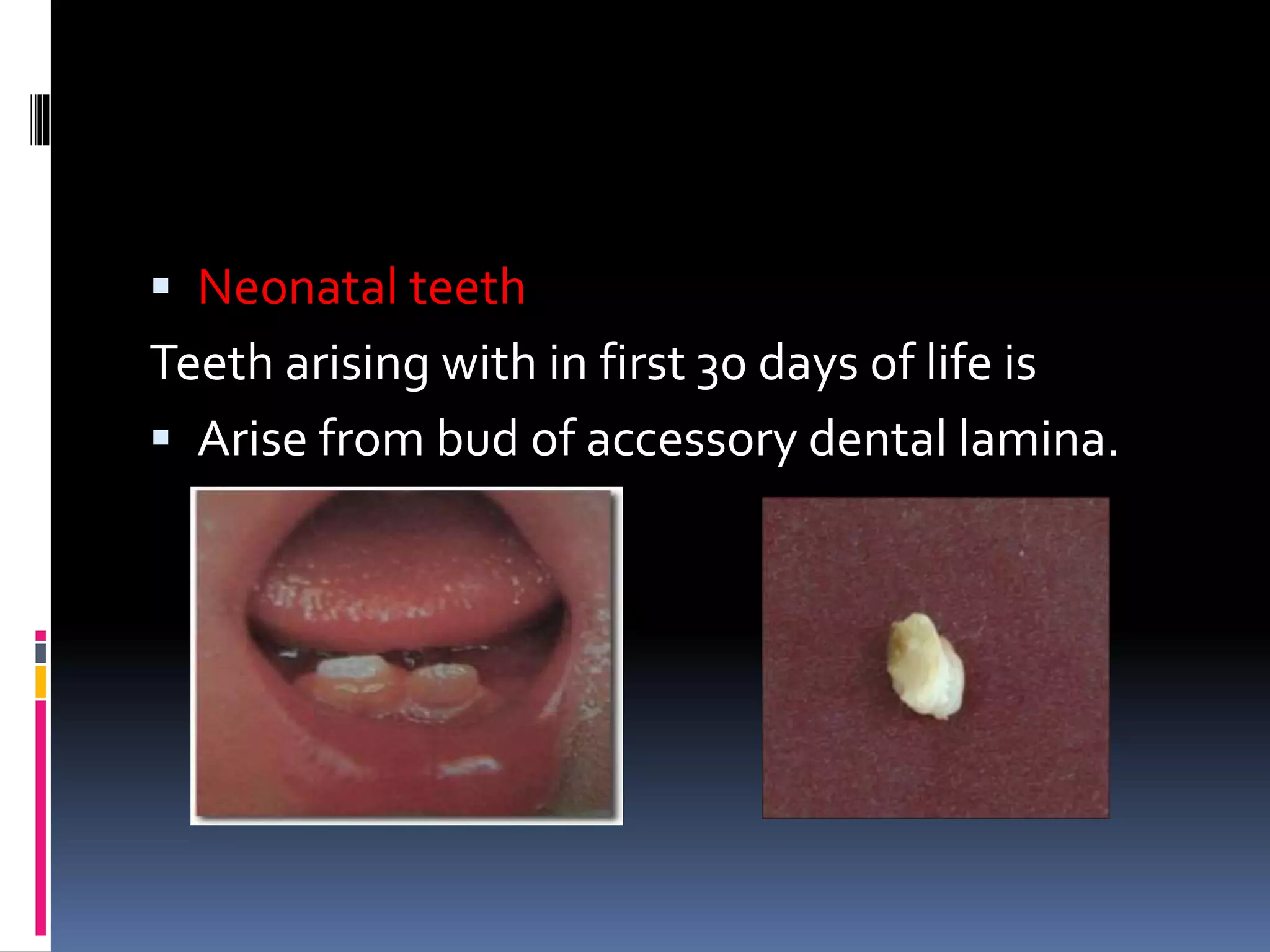
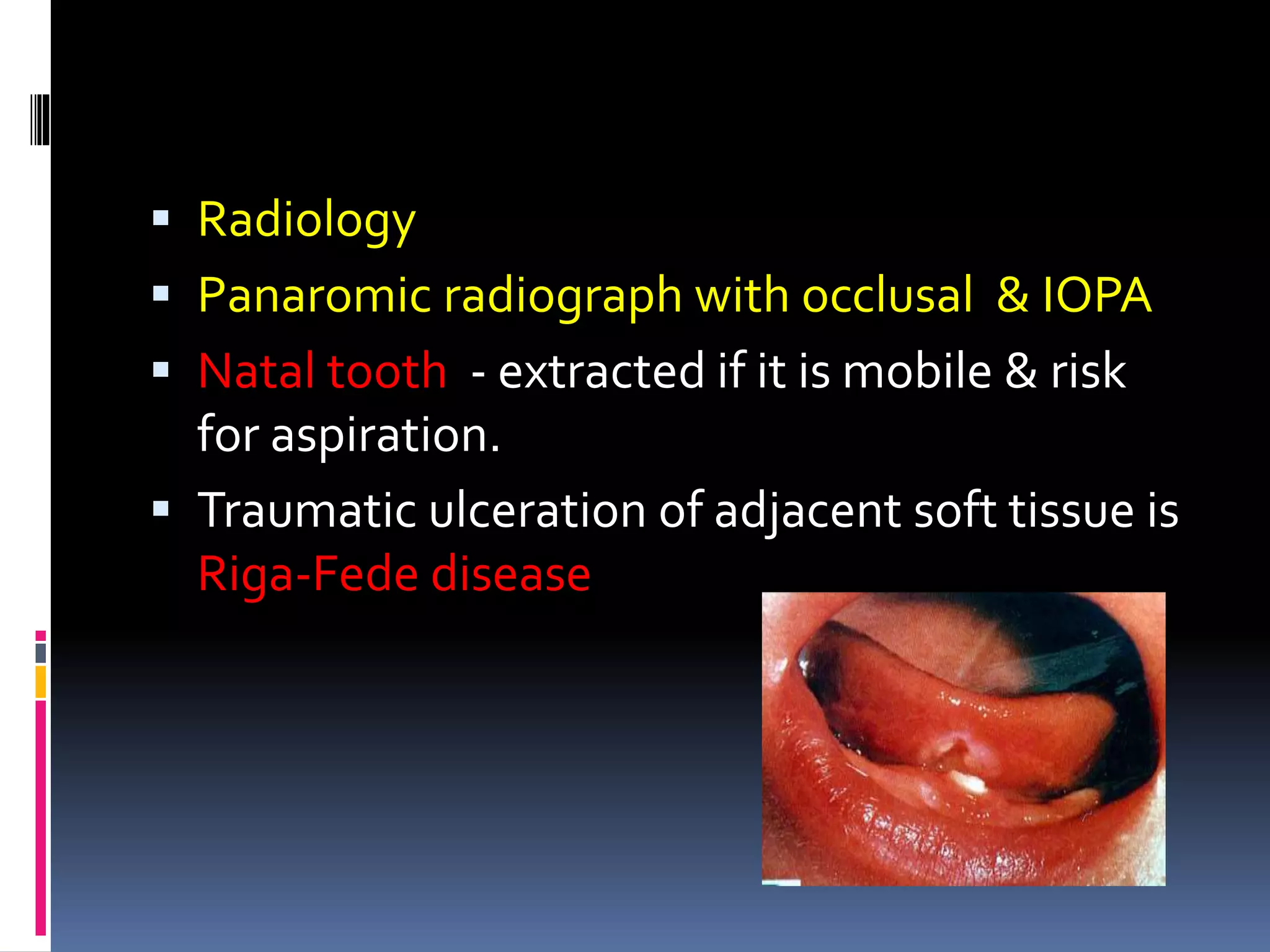
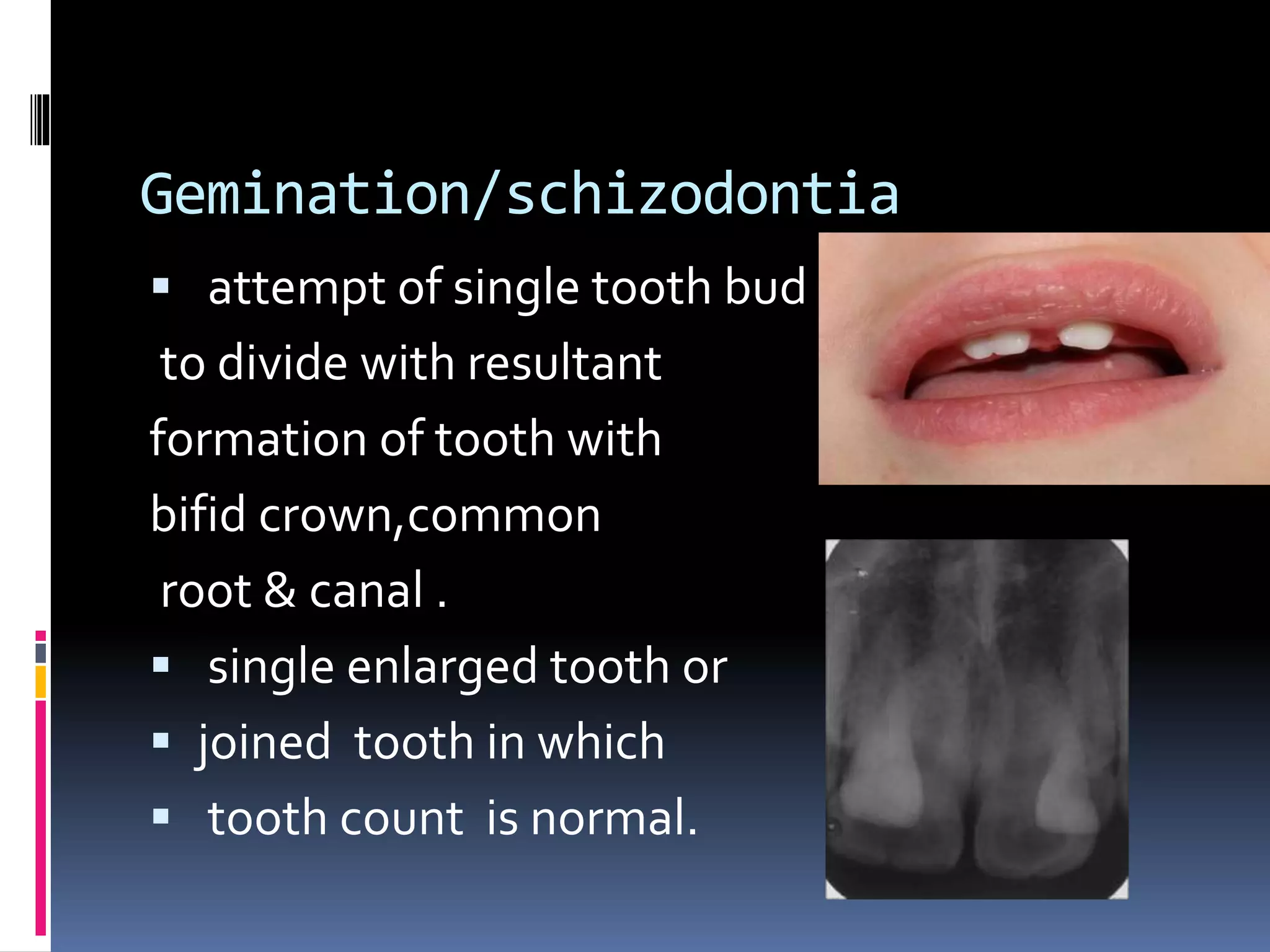
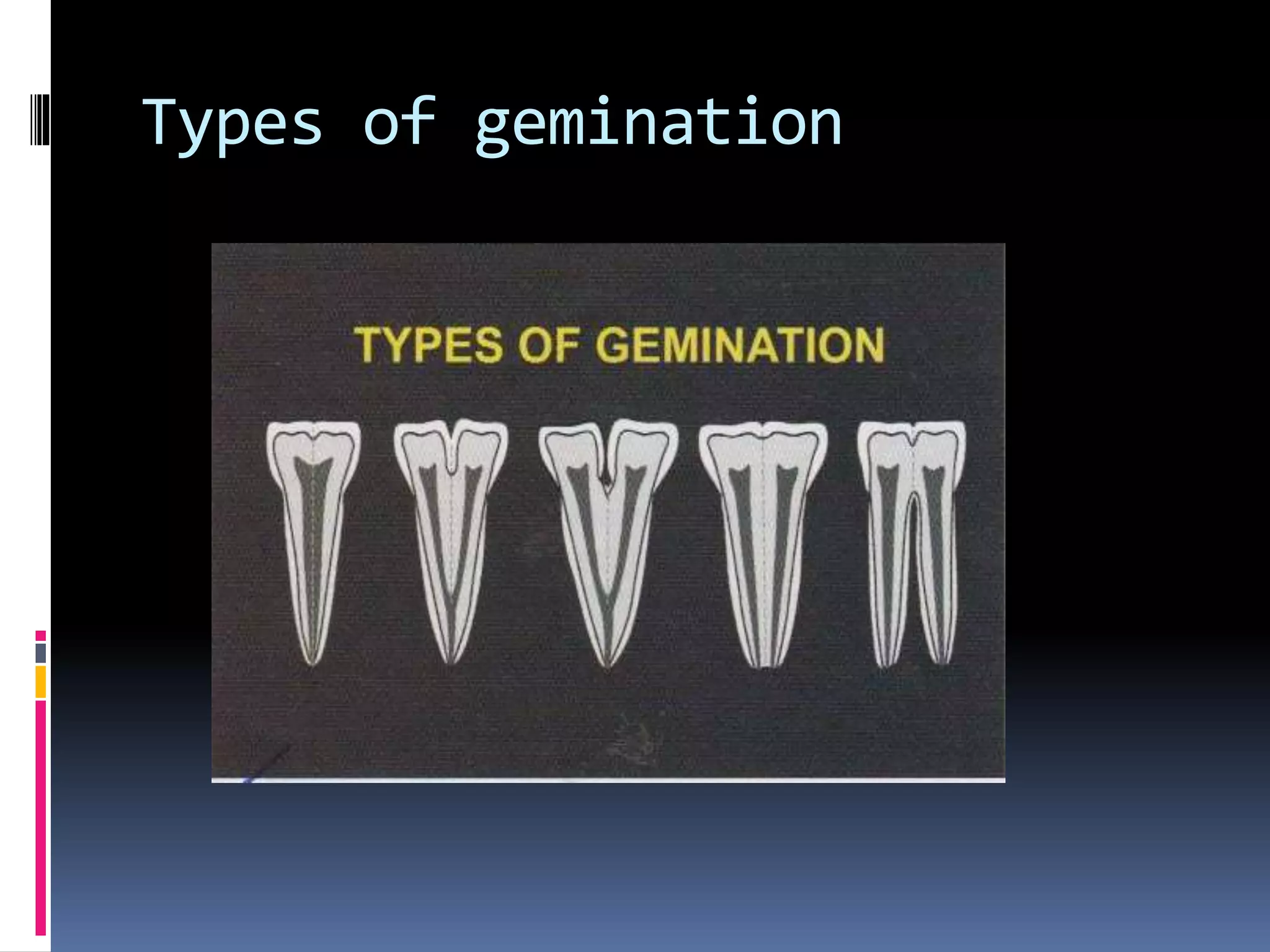
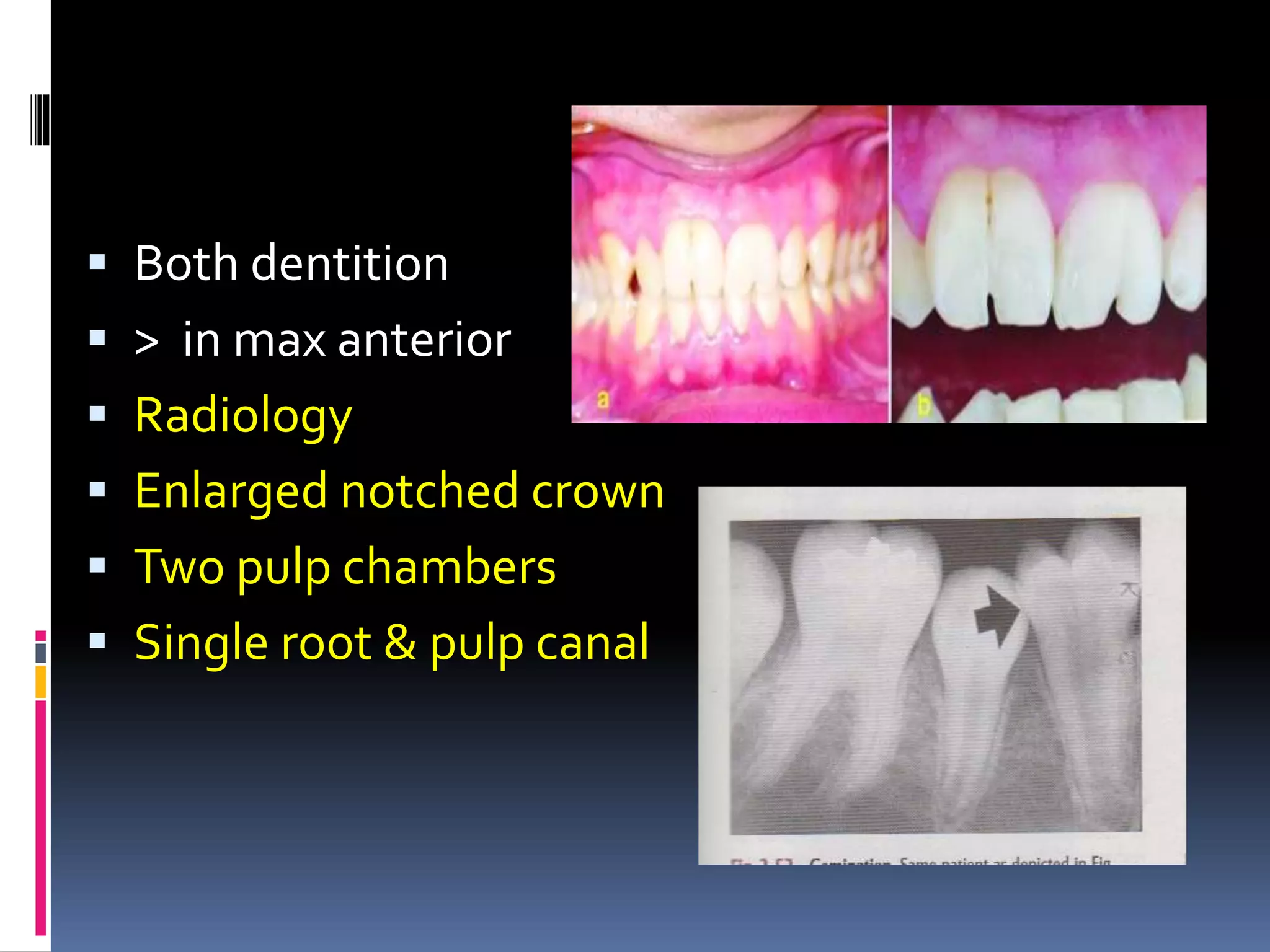
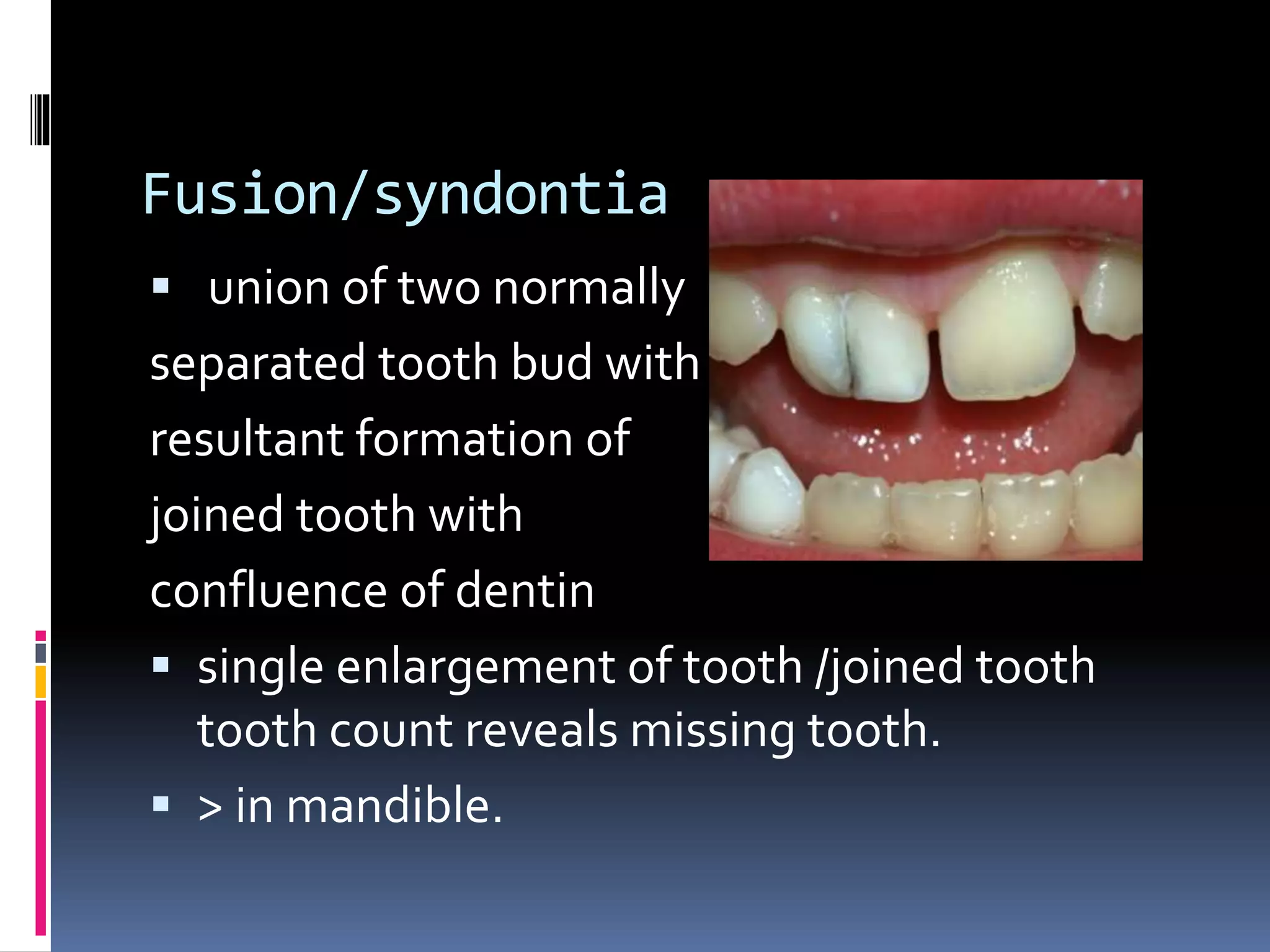
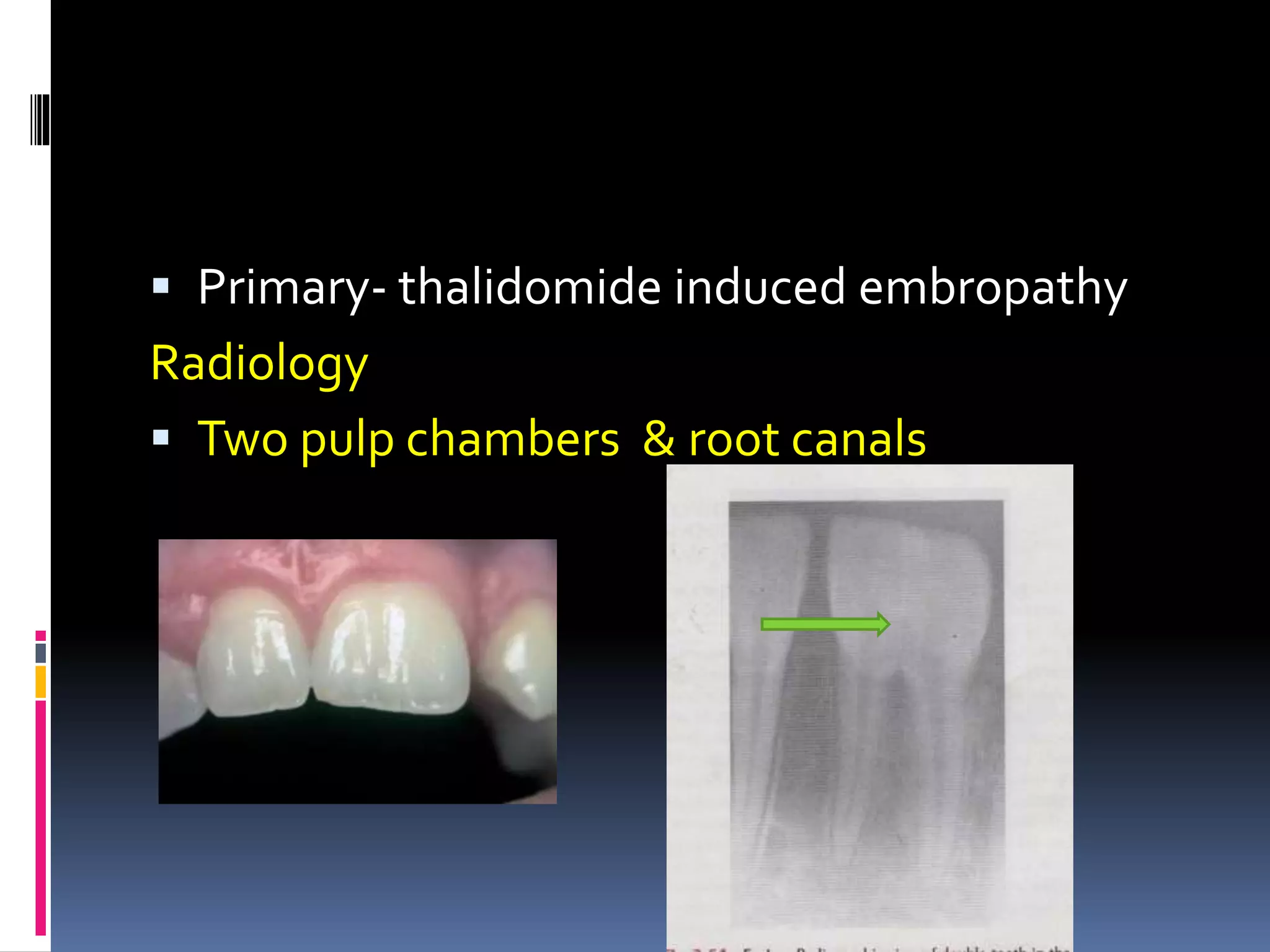
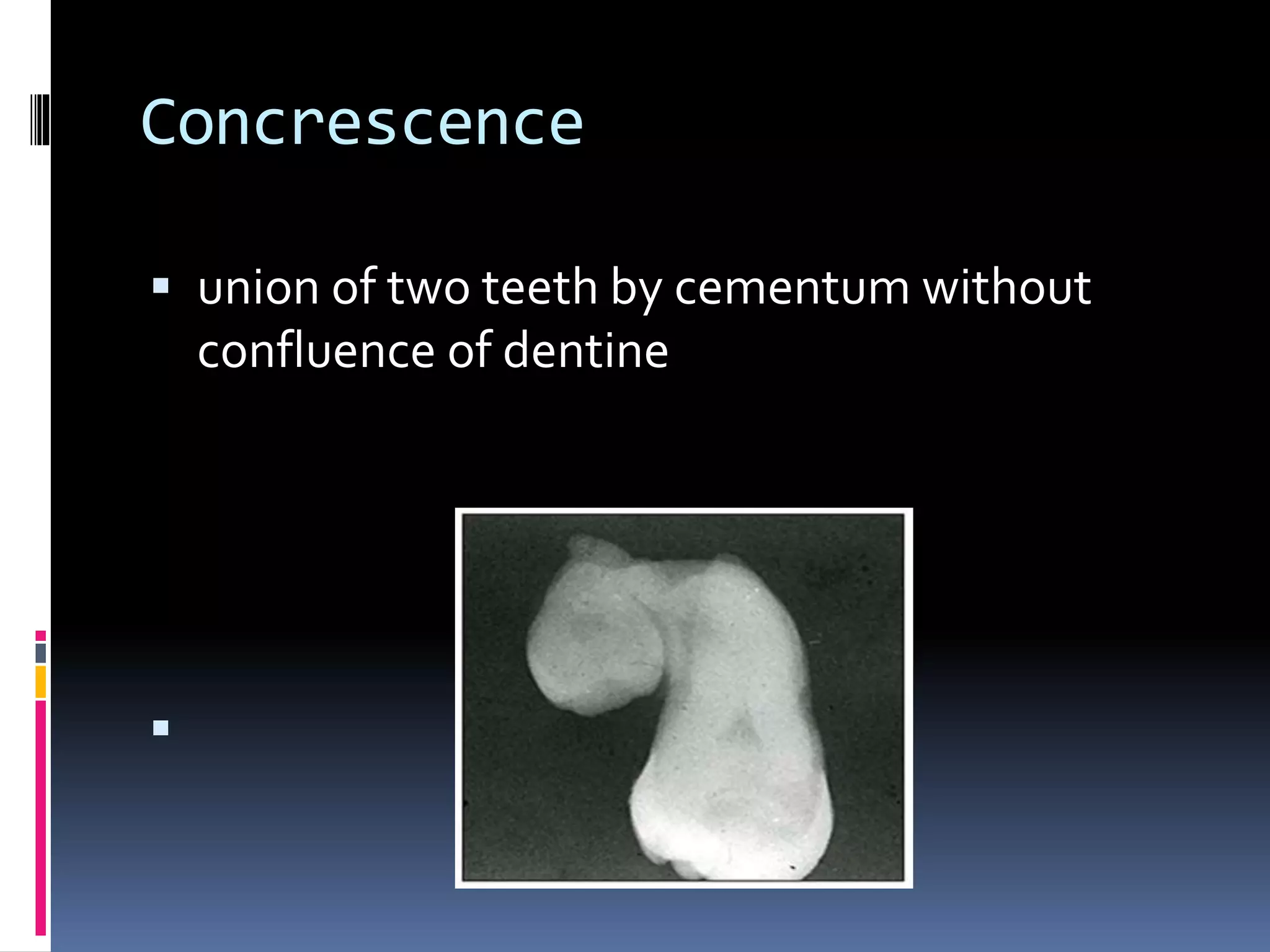
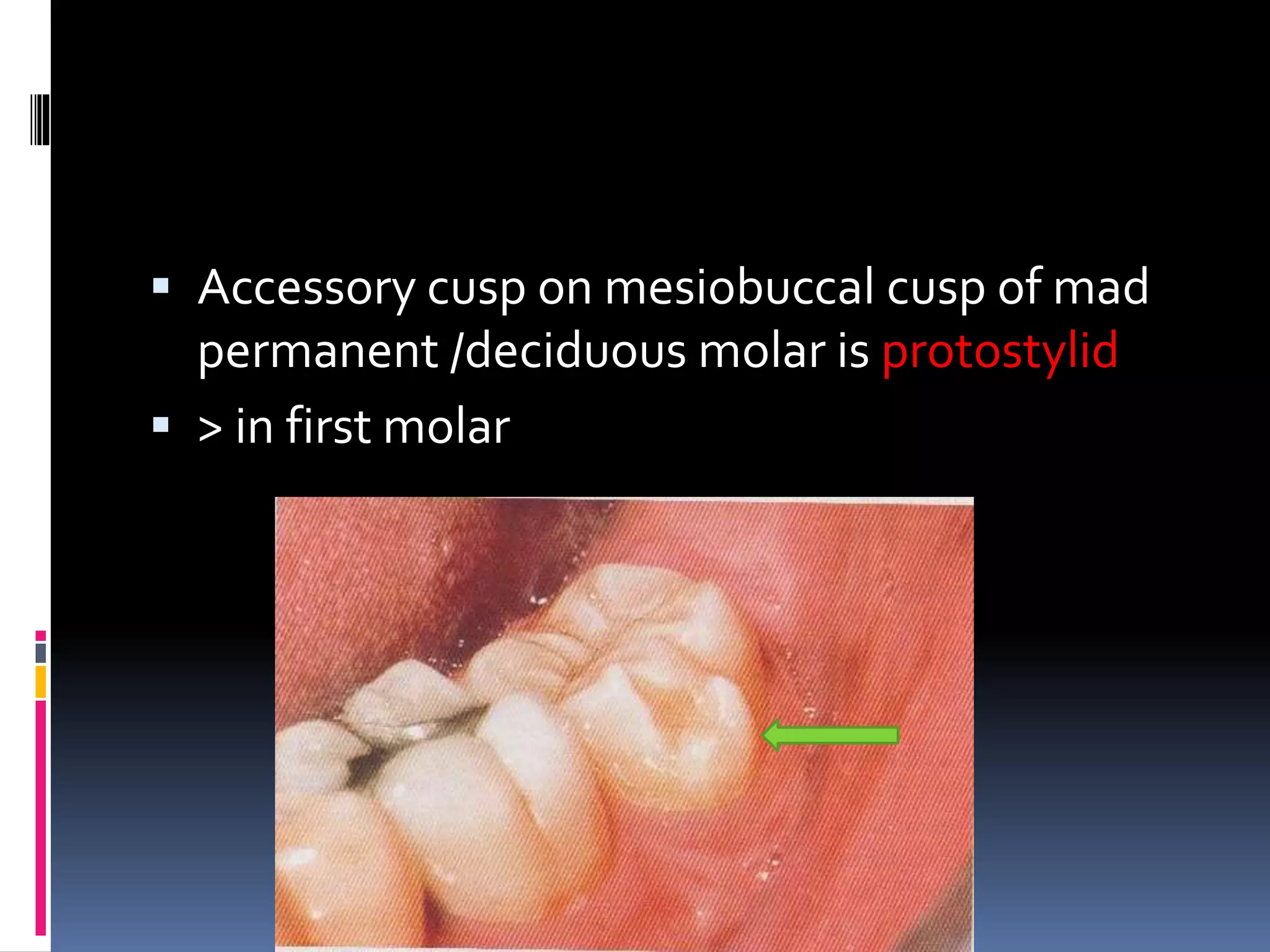
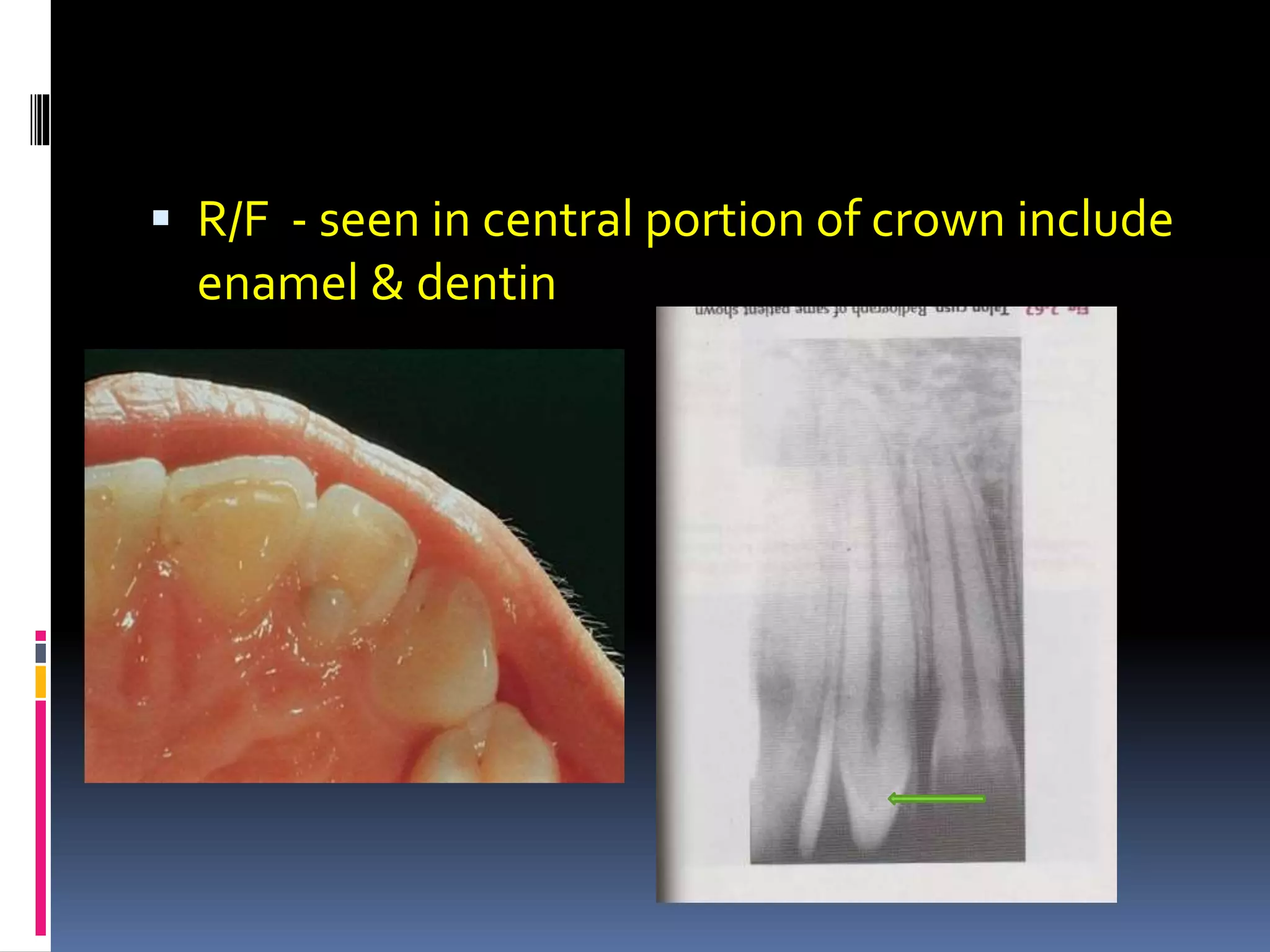
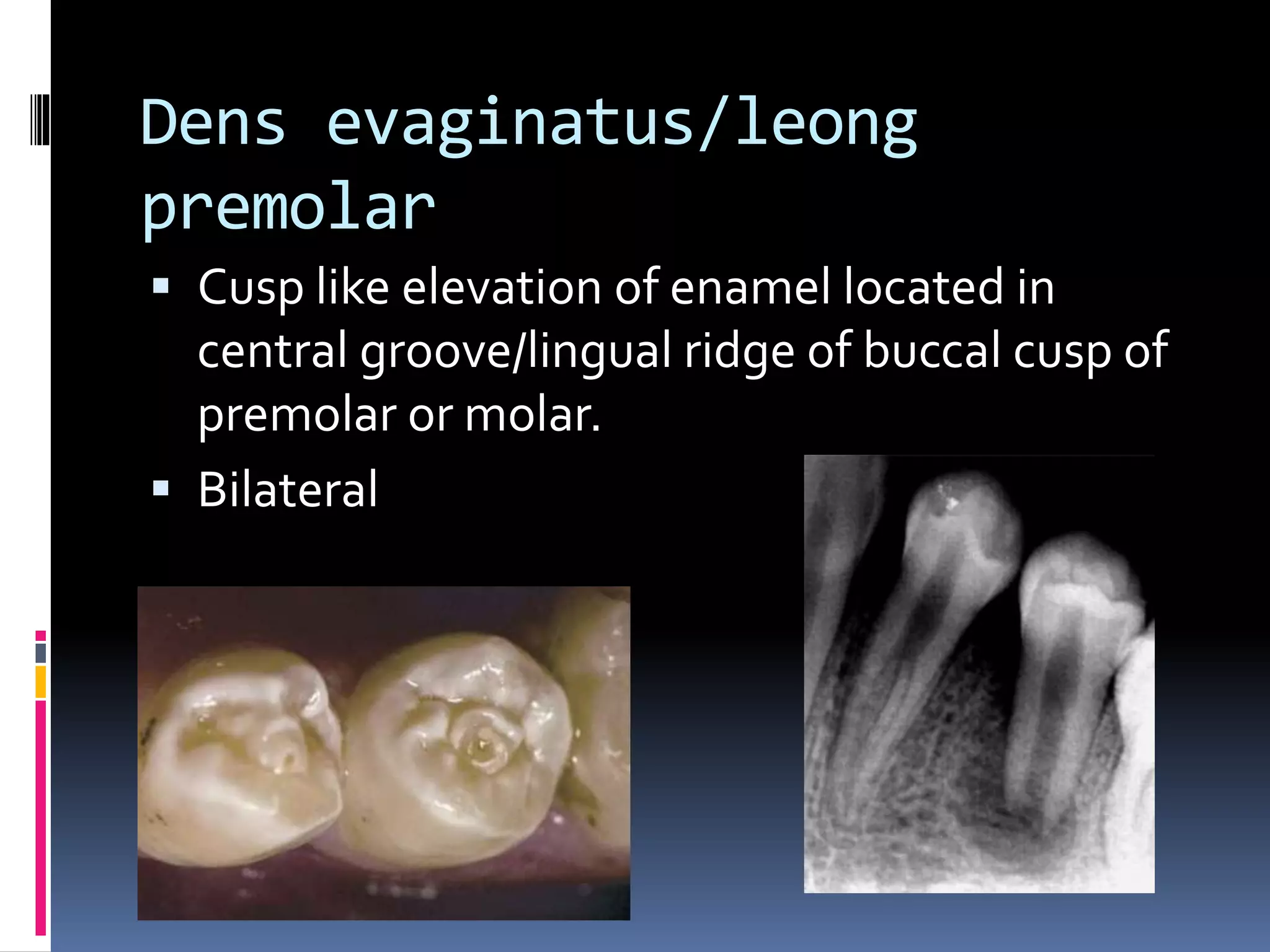
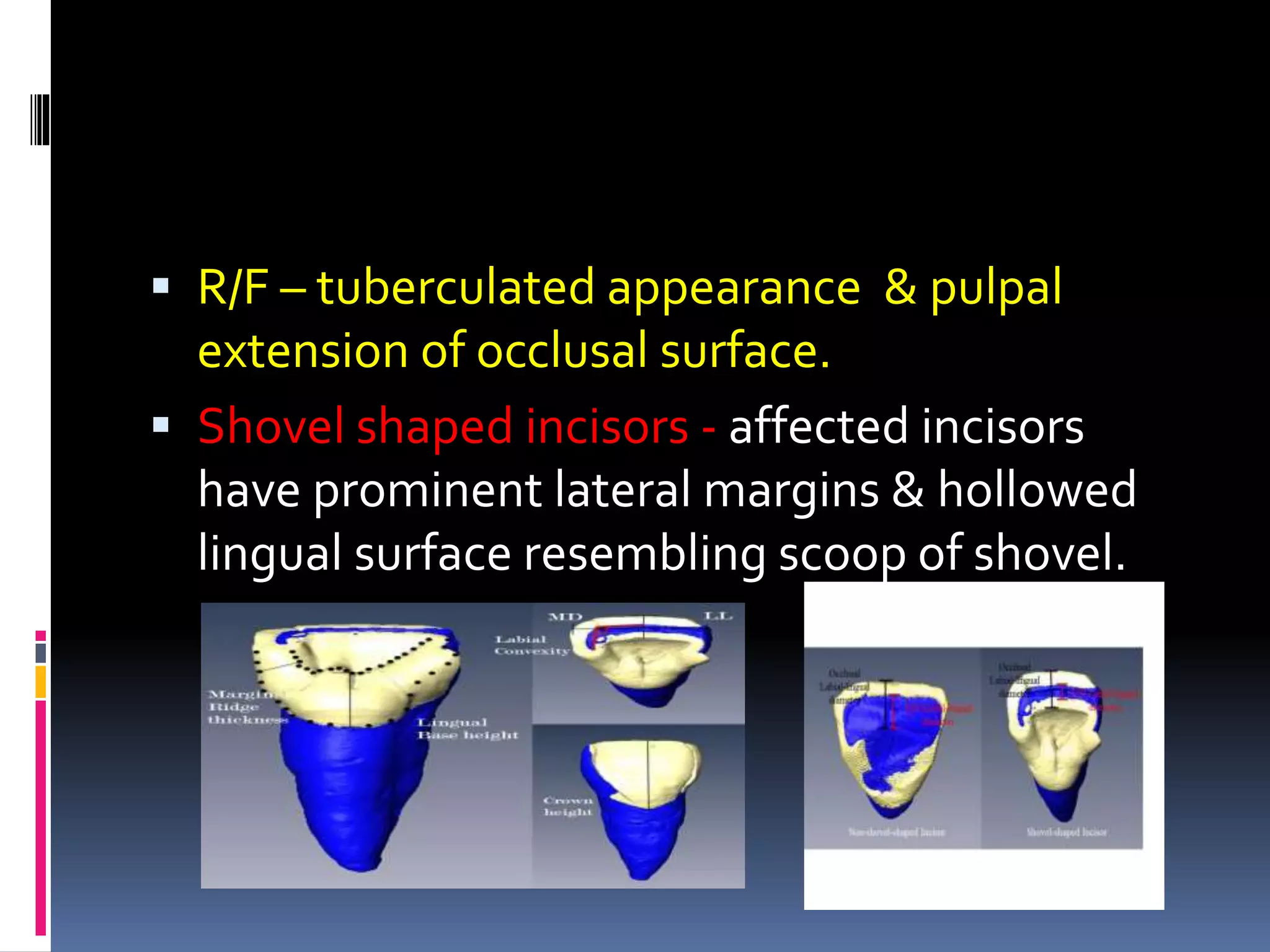
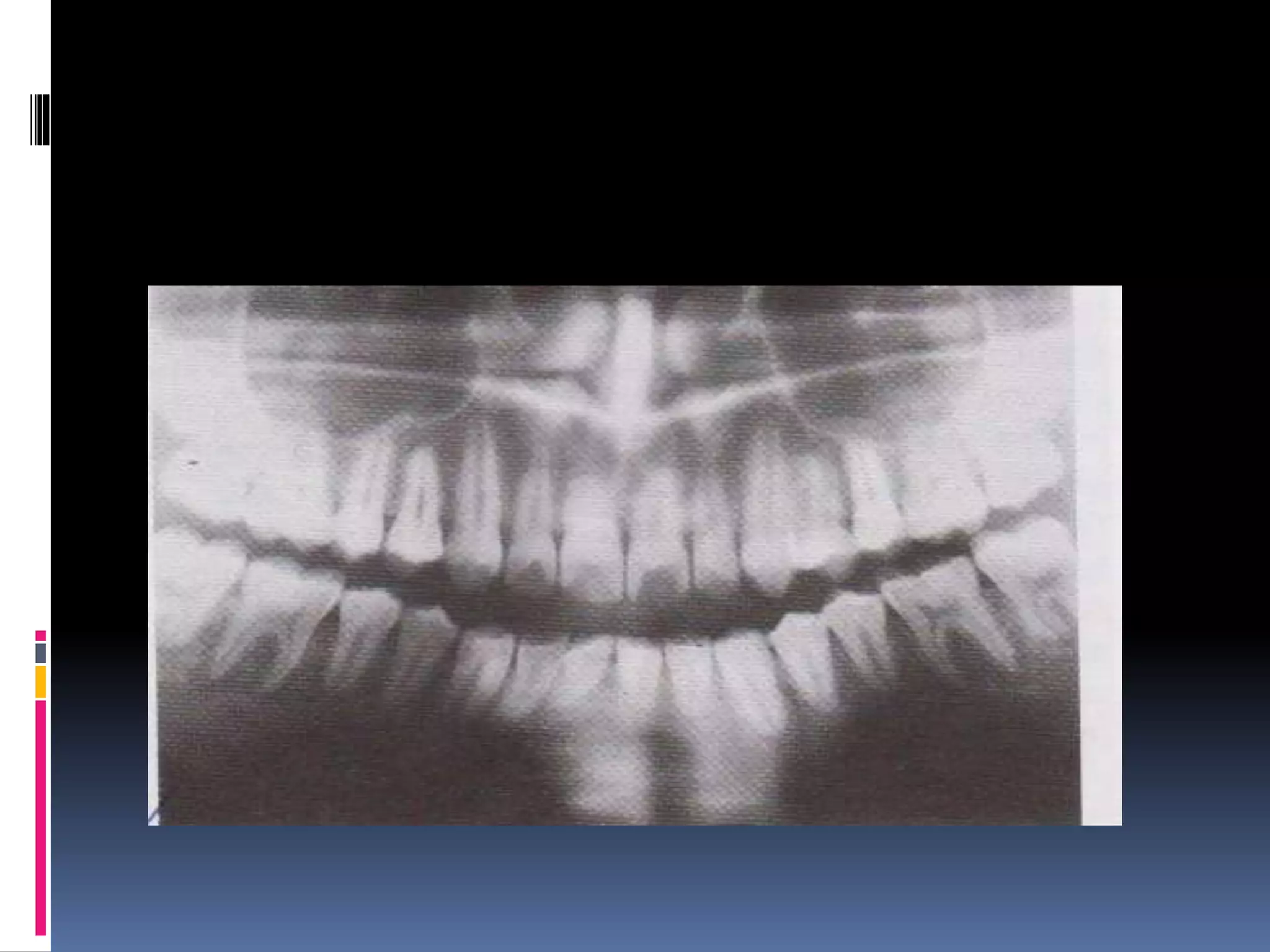
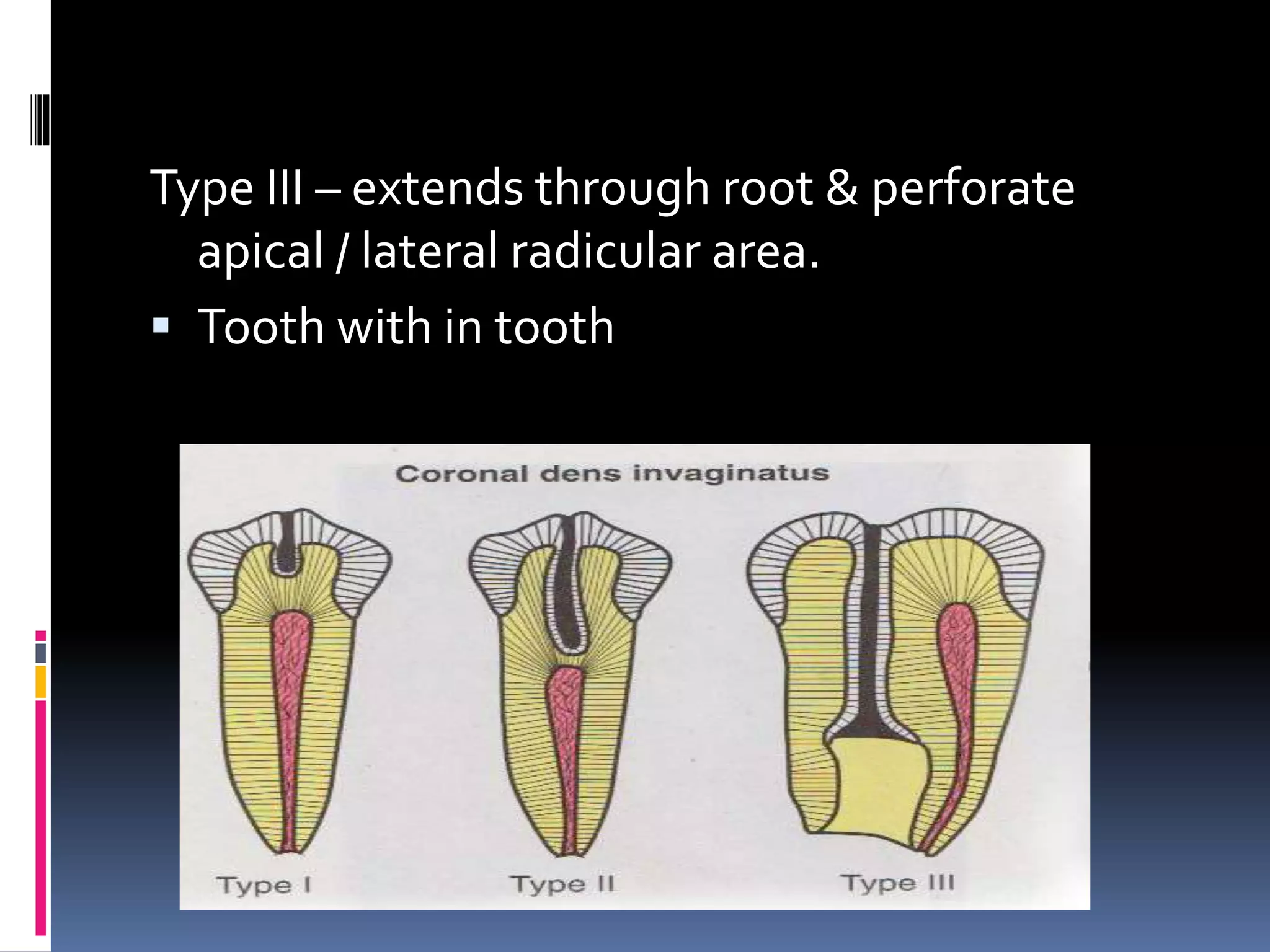
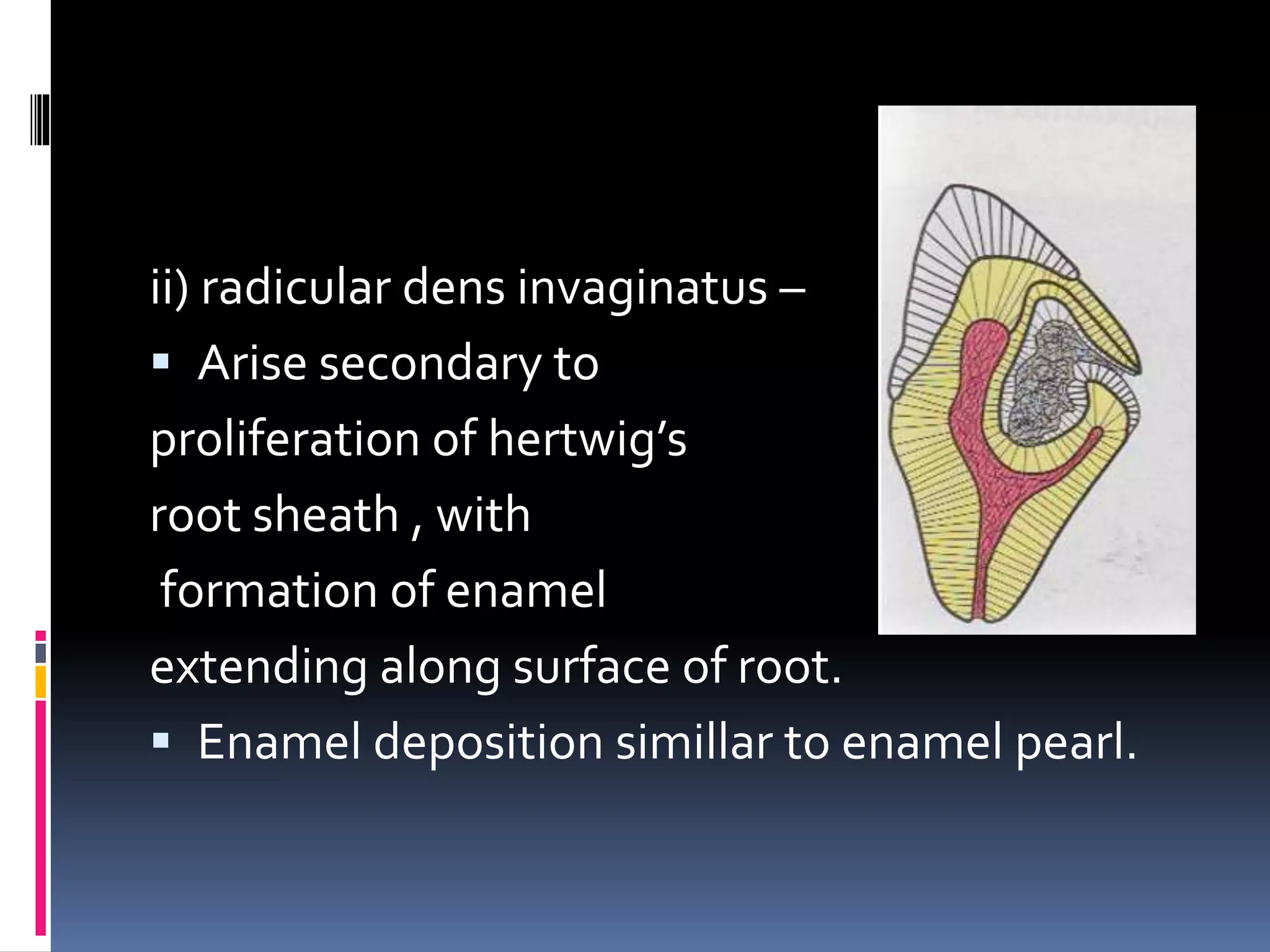
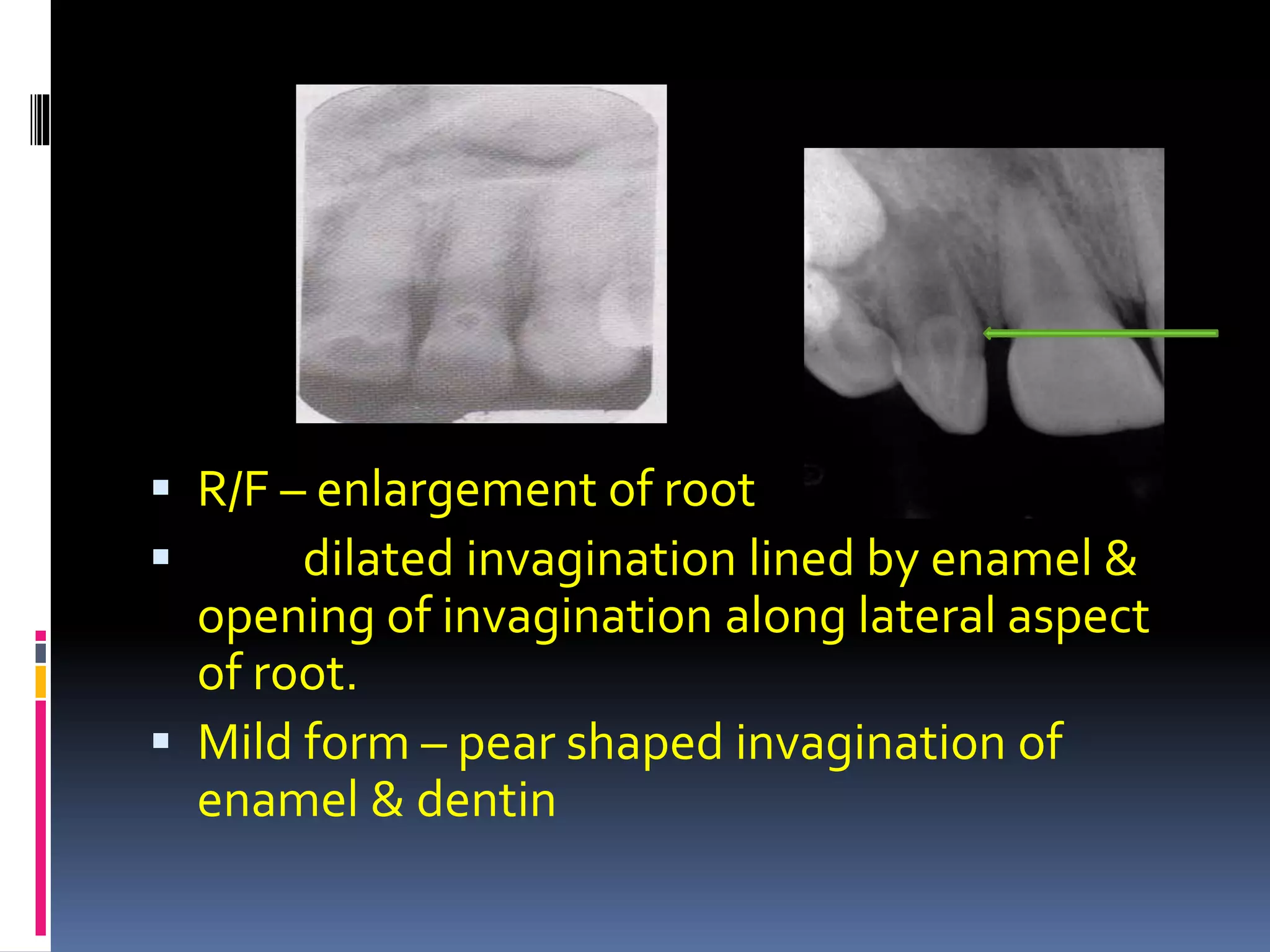
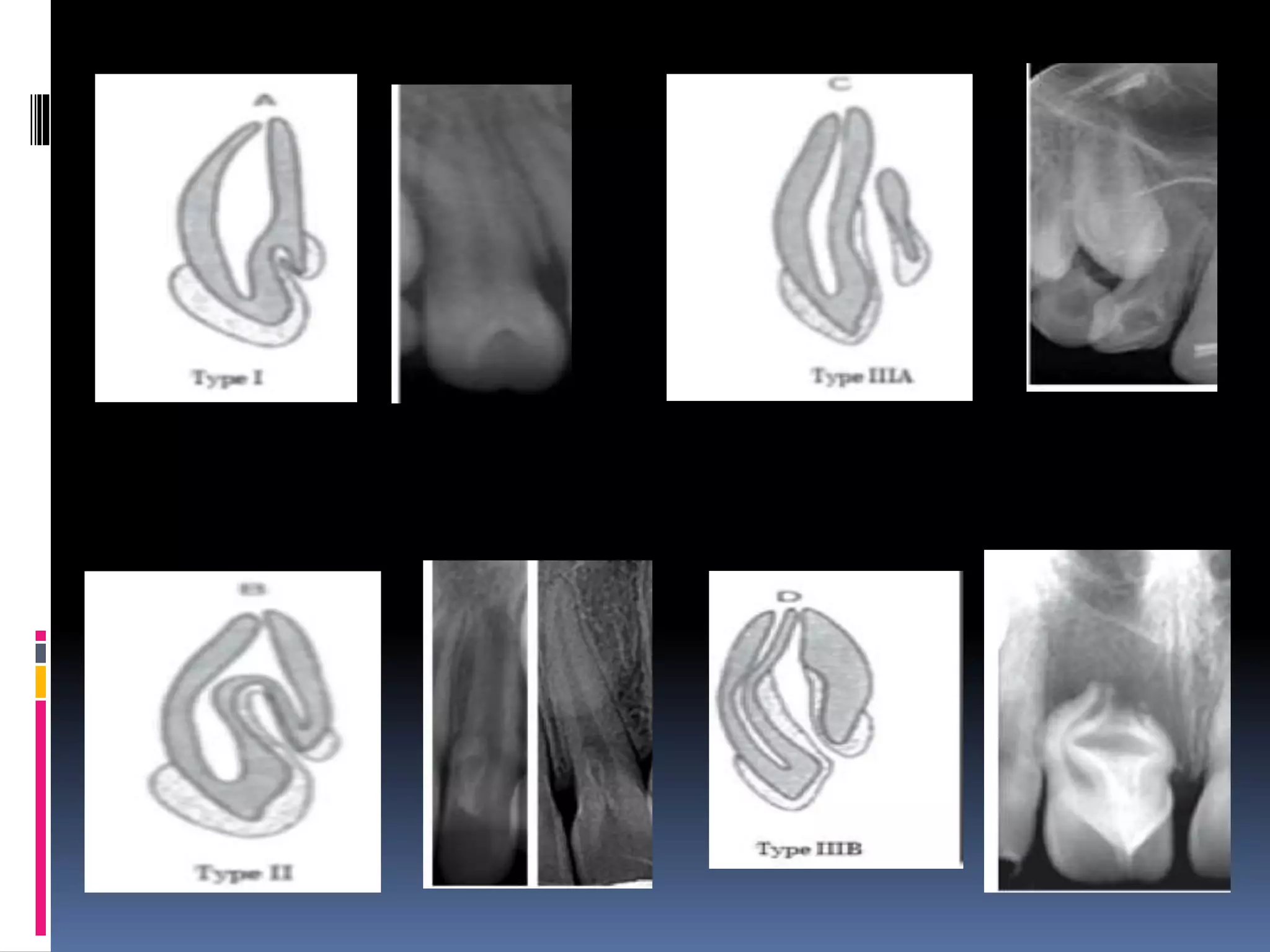
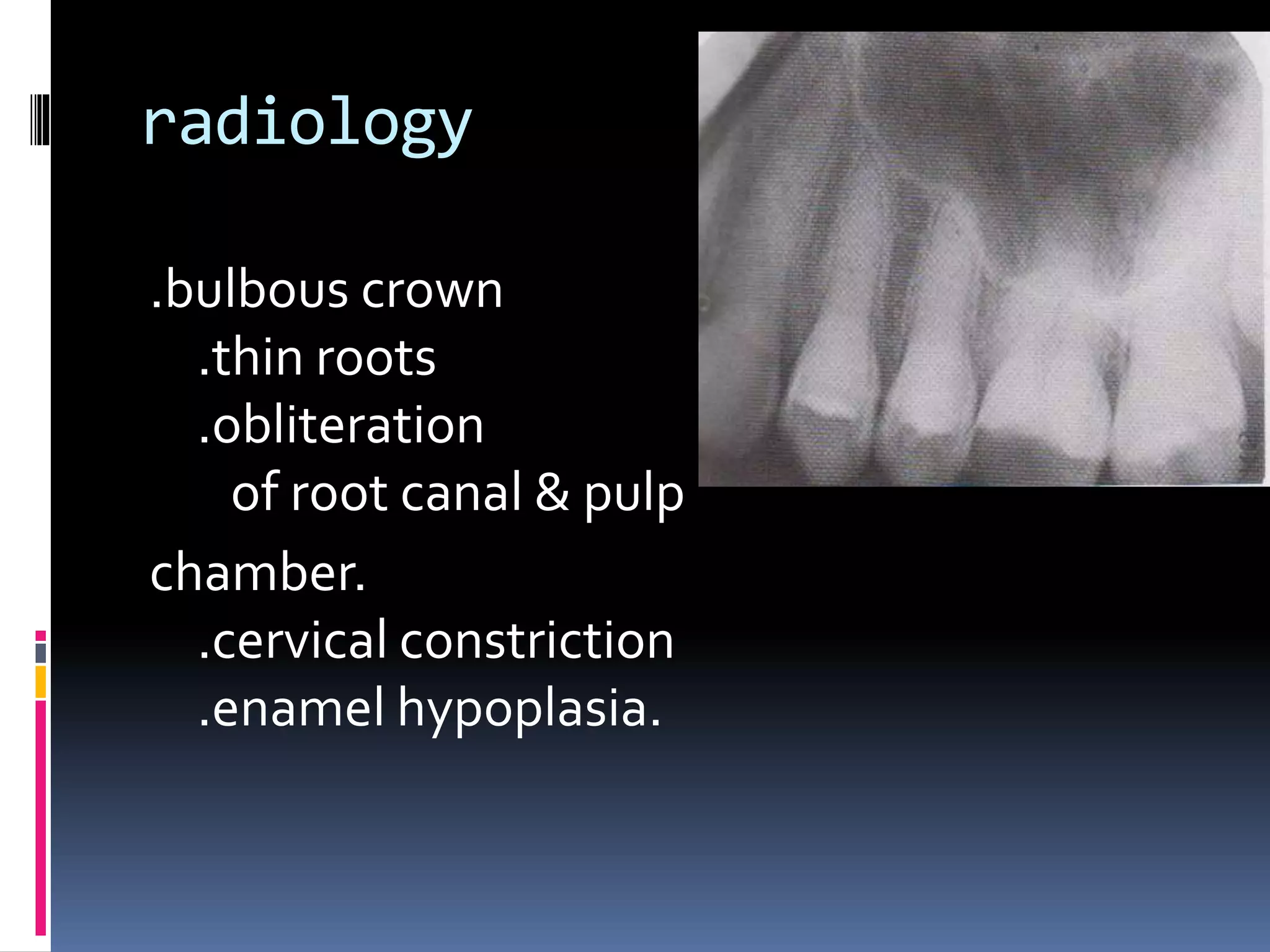
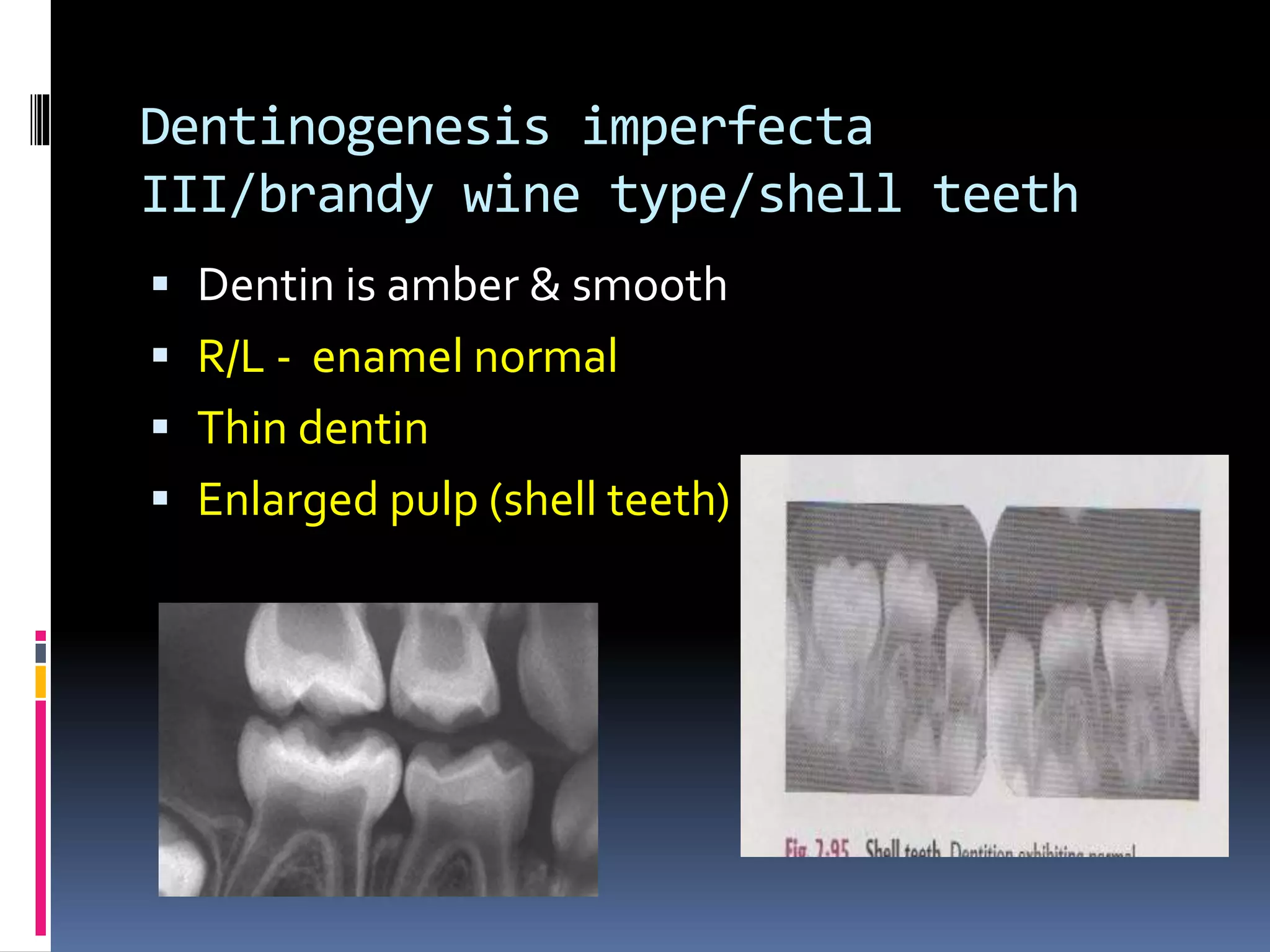
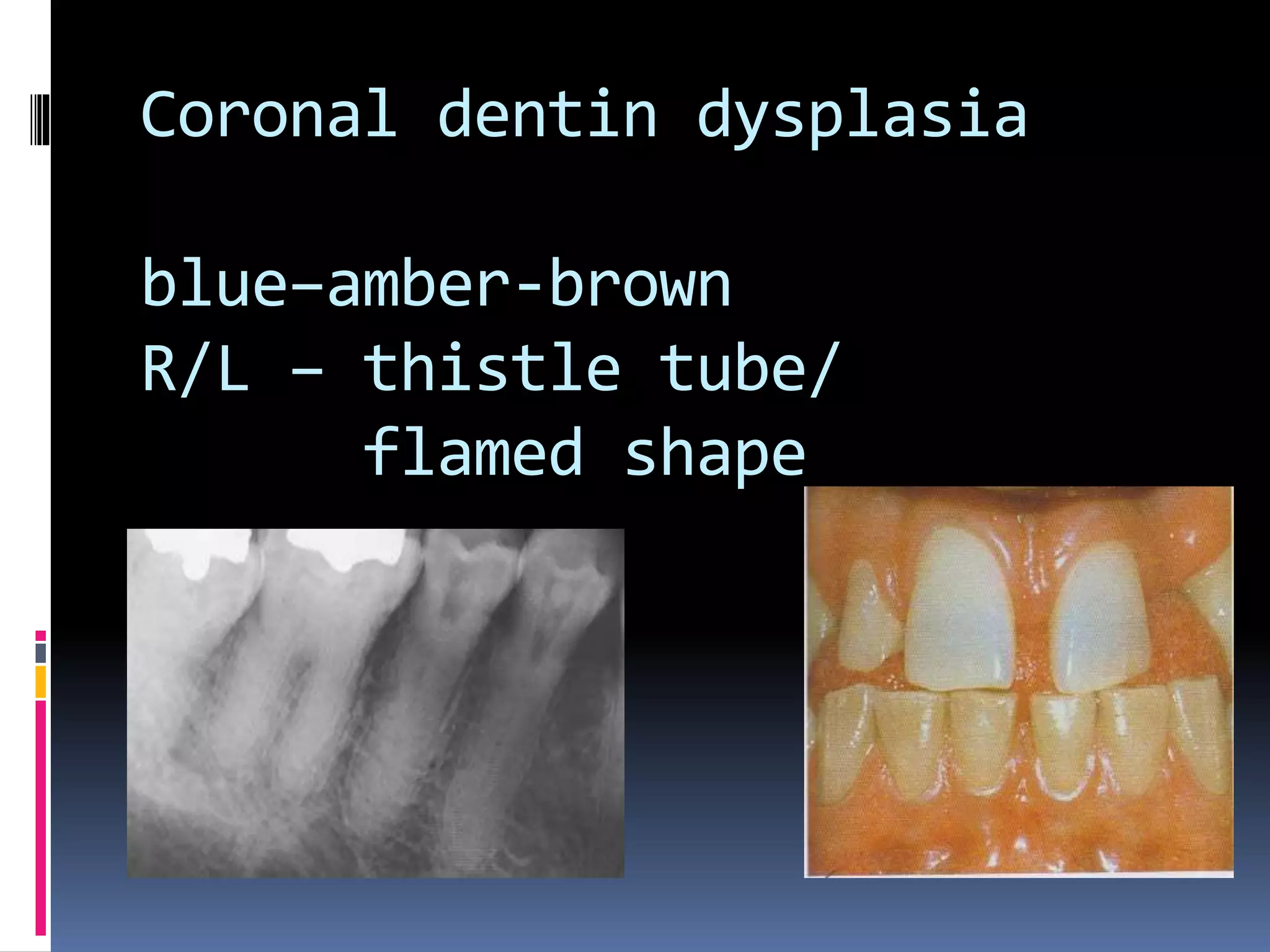
This document discusses various developmental disturbances that can affect teeth, including abnormalities in number, size, and shape. It classifies and describes conditions like hypodontia (missing teeth), hyperdontia (extra teeth), microdontia, macrodontia, gemination, fusion, dens invaginatus, and others. For each type of disturbance, it covers clinical features, radiographic findings, associated syndromes, and recommendations for treatment and prognosis. Overall, the document provides a comprehensive overview of developmental disturbances that can impact odontogenesis.