Downloaded 39 times












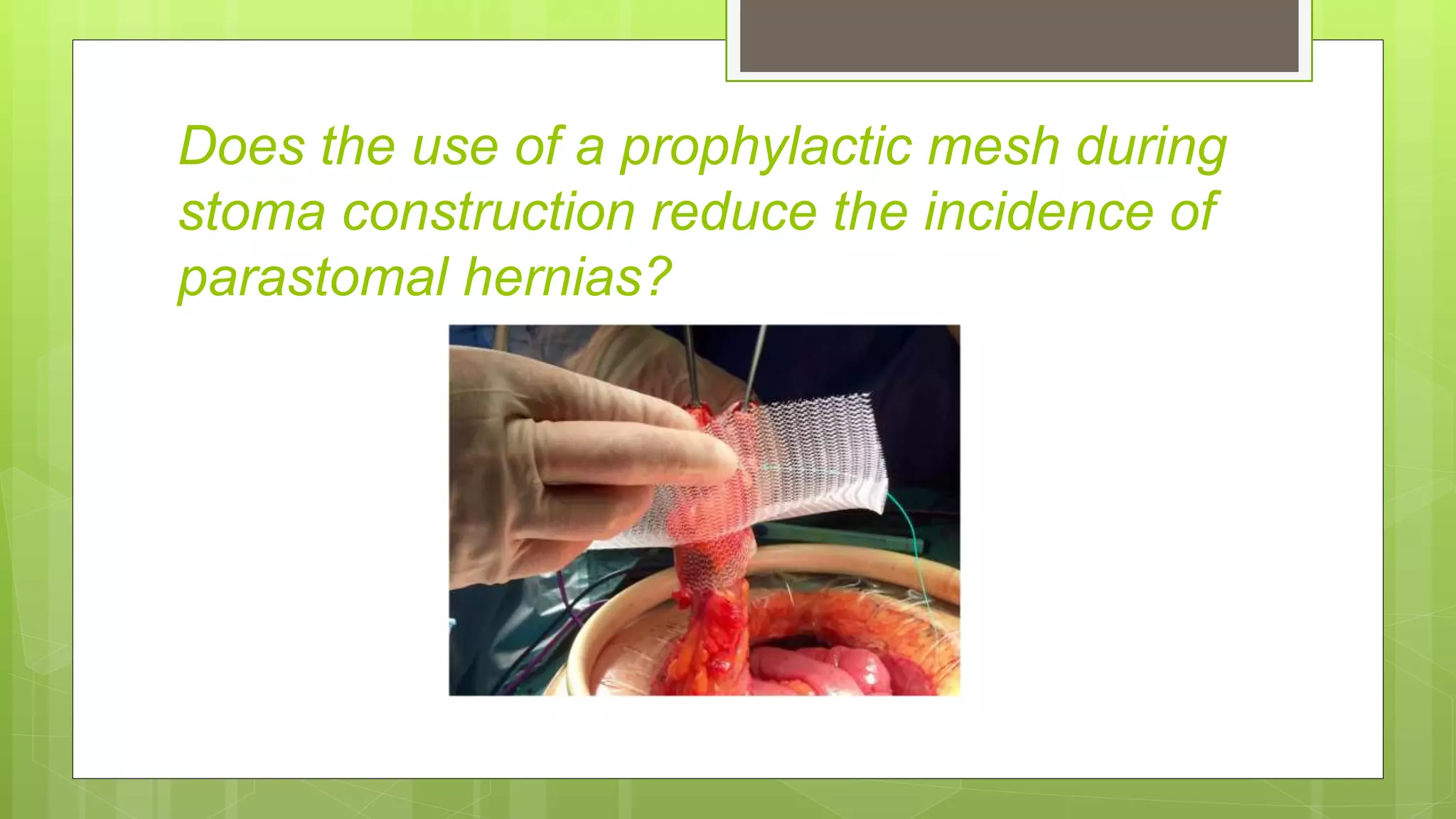










































The document discusses guidelines for the prevention and treatment of parastomal hernias. It finds that the incidence of parastomal hernias is 30-50% depending on follow up time, with terminal colostomies having a higher risk than lateral colostomies or ileostomies. Risk factors include age, obesity, infection and surgical technique. Mesh repair during hernia surgery results in lower recurrence rates of 7-17% compared to 69.4% for primary suture repair. Laparoscopic and open intraperitoneal mesh techniques have recurrence rates of around 10%. Prophylactic mesh placement during stoma creation may decrease hernia rates.



















































































