1) Acute pancreatitis is an inflammation of the pancreas that results from digestive enzymes activating prematurely inside the pancreas. The two most common causes are alcohol abuse and gallstones. Symptoms include severe abdominal pain, nausea, vomiting, and elevated blood levels of pancreatic enzymes. Complications can include shock, respiratory failure, and infection.
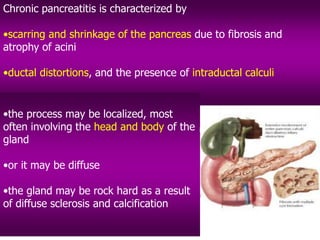
2) Chronic pancreatitis is long-standing inflammation that destroys the pancreas over time, reducing its ability to produce digestive enzymes. It commonly results from recurrent acute pancreatitis, alcoholism, or gallstones. Symptoms include abdominal pain and digestive problems like steatorrhea from reduced enzyme production.
3) Both conditions involve inflammation and damage to the pancreas from premature











![Pleuropulmonary Complications:
Pleuropulmonary complications include
•pleural effusion,
•pulmonary edema,
•respiratory failure - acute respiratory distress syndrome [ARDS]
•The effusion may be secondary to a direct effect of the inflamed, swollen
pancreas on the pleura abutting the diaphragm or to tracking of exudative fluid
from the pancreatic bed retroperitoneally into the pleural cavity through defects
in the diaphragm
•The pleural fluid is an exudate with high protein, LDH, and
amylase levels](https://image.slidesharecdn.com/pancreatitis-231114061936-02324758/85/Pancreatitis-ppt-17-320.jpg)