Downloaded 62 times
![Type I Diabetes Mellitus IDDM
b cells of the islets of Langerhans are destroyed by autoimmune
attack which may be provoked by environmental agent.
Glucose cannot enter the adipose cells.
Increased blood [glucagon].
TYPE II DIABETES MELLITUS NIDDM
Slow to develop.
Genetic factors are significant.
Occurs most often in people who are overweight.
Decreased sensitivity to insulin or an insulin resistance.
GESTATIONAL DIABETES
Some pregnant women require more insulin than their body can
produce.
IMPAIRED GLUCOSE TOLERANCE AND PREDIABETES
It is a condition in which blood glucose levels are higher than
normal but not high enough for a diagnosis of diabetes. Patients
are at high risk of developing type 2 diabetes.
INSULINOMA](https://image.slidesharecdn.com/pancreas-141014151859-conversion-gate01/85/Pancreas-10-320.jpg)

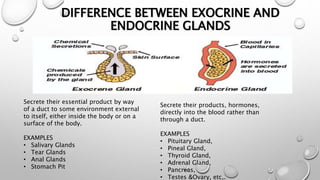
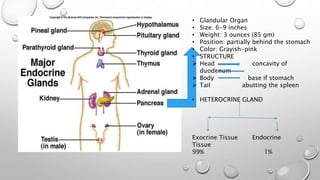
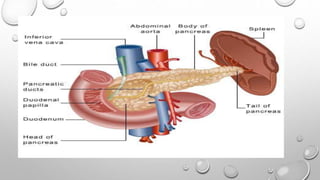
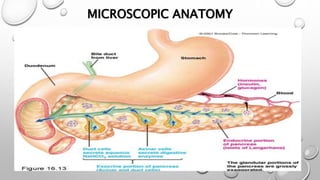
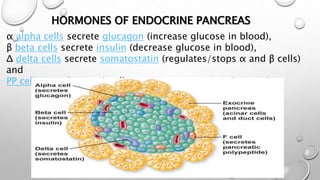
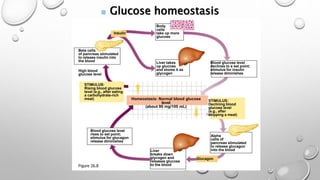
The document discusses the endocrine pancreas and its role in regulating blood glucose levels. It notes that the pancreas has both exocrine and endocrine functions. The endocrine pancreas contains four main cell types - alpha, beta, delta, and PP cells. Alpha cells secrete glucagon, which raises blood glucose levels. Beta cells secrete insulin, which lowers blood glucose levels. Delta cells secrete somatostatin, which regulates alpha and beta cell secretion. PP cells secrete pancreatic polypeptide, though its role is uncertain. Together, glucagon and insulin work to maintain glucose homeostasis and keep blood glucose levels within a normal range.



































































