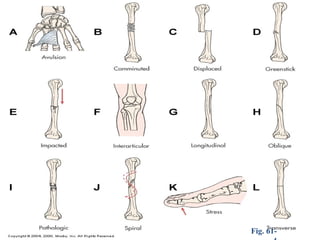
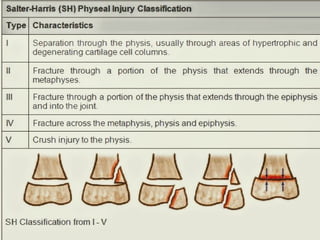
The document discusses fractures in children, detailing types, causes, classifications (like Salter-Harris), and healing processes. It highlights the differences between children's and adults' bones, emphasizing specific fractures such as greenstick and buckle. Management strategies include first aid techniques and hospital treatments, which focus on reducing and immobilizing fractures to restore function.