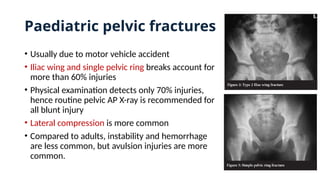
Paediatric pelvic fractures
•Usually due to motor vehicle accident
• Iliac wing and single pelvic ring breaks account for
more than 60% injuries
• Physical examination detects only 70% injuries,
hence routine pelvic AP X-ray is recommended for
all blunt injury
• Lateral compression is more common
• Compared to adults, instability and hemorrhage
are less common, but avulsion injuries are more
common.
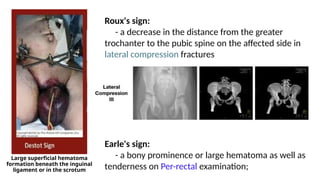
Large superficial hematoma
formationbeneath the inguinal
ligament or in the scrotum
Roux's sign:
- a decrease in the distance from the greater
trochanter to the pubic spine on the affected side in
lateral compression fractures
Earle's sign:
- a bony prominence or large hematoma as well as
tenderness on Per-rectal examination;
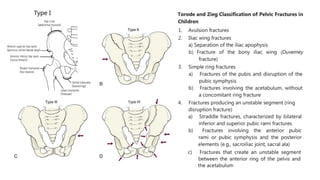
5.
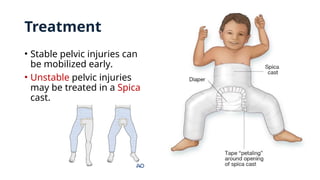
Treatment
• Stable pelvicinjuries can
be mobilized early.
• Unstable pelvic injuries
may be treated in a Spica
cast.
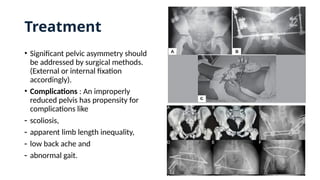
6.
• Significant pelvicasymmetry should
be addressed by surgical methods.
(External or internal fixation
accordingly).
• Complications : An improperly
reduced pelvis has propensity for
complications like
- scoliosis,
- apparent limb length inequality,
- low back ache and
- abnormal gait.
Treatment
7.
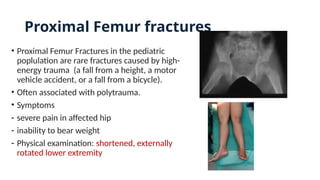
Proximal Femur fractures
•Proximal Femur Fractures in the pediatric
poplulation are rare fractures caused by high-
energy trauma (a fall from a height, a motor
vehicle accident, or a fall from a bicycle).
• Often associated with polytrauma.
• Symptoms
- severe pain in affected hip
- inability to bear weight
- Physical examination: shortened, externally
rotated lower extremity
9.
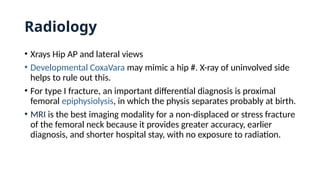
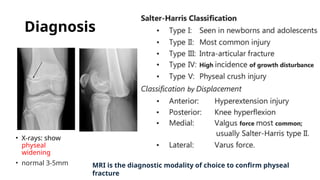
Radiology
• Xrays HipAP and lateral views
• Developmental CoxaVara may mimic a hip #. X-ray of uninvolved side
helps to rule out this.
• For type I fracture, an important differential diagnosis is proximal
femoral epiphysiolysis, in which the physis separates probably at birth.
• MRI is the best imaging modality for a non-displaced or stress fracture
of the femoral neck because it provides greater accuracy, earlier
diagnosis, and shorter hospital stay, with no exposure to radiation.
10.
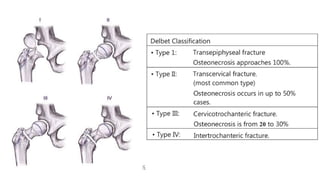
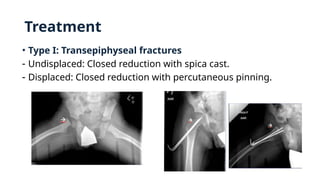
Treatment
• Type I:Transepiphyseal fractures
- Undisplaced: Closed reduction with spica cast.
- Displaced: Closed reduction with percutaneous pinning.
11.
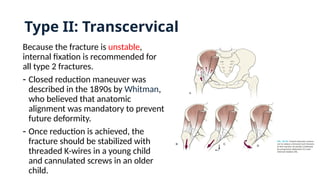
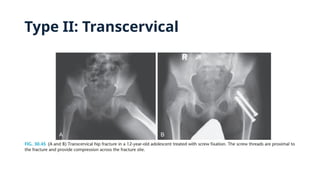
Type II: Transcervical
Becausethe fracture is unstable,
internal fixation is recommended for
all type 2 fractures.
- Closed reduction maneuver was
described in the 1890s by Whitman,
who believed that anatomic
alignment was mandatory to prevent
future deformity.
- Once reduction is achieved, the
fracture should be stabilized with
threaded K-wires in a young child
and cannulated screws in an older
child.
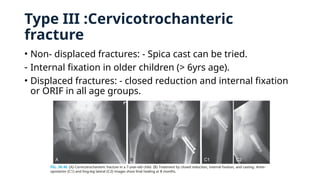
Type III :Cervicotrochanteric
fracture
•Non- displaced fractures: - Spica cast can be tried.
- Internal fixation in older children (> 6yrs age).
• Displaced fractures: - closed reduction and internal fixation
or ORIF in all age groups.
14.
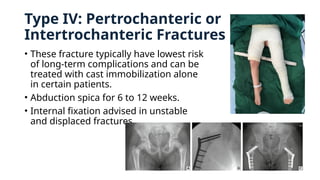
Type IV: Pertrochantericor
Intertrochanteric Fractures
• These fracture typically have lowest risk
of long-term complications and can be
treated with cast immobilization alone
in certain patients.
• Abduction spica for 6 to 12 weeks.
• Internal fixation advised in unstable
and displaced fractures.
15.
Points to beconsidered while treating a paediatric hip fracture
• Consider hip joint aspiration when a fracture is treated closed so that the
tamponade effect is relieved.
• Avoid compromise of fracture stability/fixation in order to protect the physis;
cross the physis when necessary to achieve stability.
• Internal fixation options:
- 0 to 3 yrs age: smooth pins(2/2.4mm)or cannulated screws (3.5/4.0mm)
- 4 to 8 yrs age:cannulated screws (4/4.5mm) or a paediatric hip-compression
screw.
- > 8 yrs: cannulated screws (6.5/7.3mm) or a hip compression screw
• Pediatric bone is often denser than adult, hence consider pre-drilling.
• Consider using an additional hip spica cast in < 8 years
16.
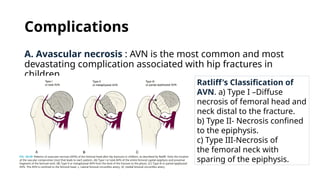
Complications
A. Avascular necrosis: AVN is the most common and most
devastating complication associated with hip fractures in
children.
Ratliff's Classification of
AVN. a) Type I –Diffuse
necrosis of femoral head and
neck distal to the fracture.
b) Type II- Necrosis confined
to the epiphysis.
c) Type III-Necrosis of
the femoral neck with
sparing of the epiphysis.
17.
• Treatment:
- Useof an abduction orthosis
- Established AVN: Arthrodesis
- Early AVN: Core decompression and use of vascularised fibular graft have been tried
recently.
B. Premature physeal closure
- Mostly due to pins penetrating the physis
- Can cause femoral shortening, Coxavara, and short femoral neck.
C. CoxaVara
D. Nonunion: Due to inadequate reduction
- Requires a valgus intertrochanteric osteotomy
Complications
18.
Femoral shaft fractures
•In children younger than walking
age, 80% of these injuries are due to
child abuse.
• Hypotension due to isolated femoral
shaft # is rare
• Waddell's triad: head injury,
intraabdominal or intrathoracic
trauma, and femoral shaft fracture.
This is usually associated with shock.
19.
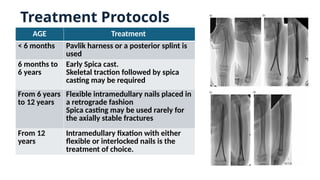
Treatment Protocols
AGE Treatment
<6 months Pavlik harness or a posterior splint is
used
6 months to
6 years
Early Spica cast.
Skeletal traction followed by spica
casting may be required
From 6 years
to 12 years
Flexible intramedullary nails placed in
a retrograde fashion
Spica casting may be used rarely for
the axially stable fractures
From 12
years
Intramedullary fixation with either
flexible or interlocked nails is the
treatment of choice.
20.
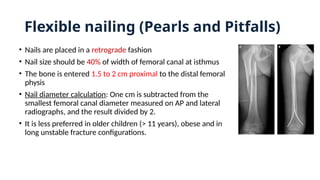
Flexible nailing (Pearlsand Pitfalls)
• Nails are placed in a retrograde fashion
• Nail size should be 40% of width of femoral canal at isthmus
• The bone is entered 1.5 to 2 cm proximal to the distal femoral
physis
• Nail diameter calculation: One cm is subtracted from the
smallest femoral canal diameter measured on AP and lateral
radiographs, and the result divided by 2.
• It is less preferred in older children (> 11 years), obese and in
long unstable fracture configurations.
21.
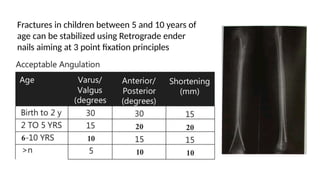
Fractures in childrenbetween 5 and 10 years of
age can be stabilized using Retrograde ender
nails aiming at 3 point fixation principles
22.
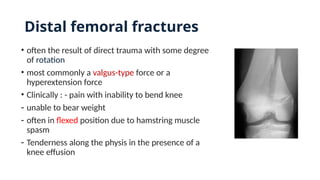
Distal femoral fractures
•often the result of direct trauma with some degree
of rotation
• most commonly a valgus-type force or a
hyperextension force
• Clinically : - pain with inability to bend knee
- unable to bear weight
- often in flexed position due to hamstring muscle
spasm
- Tenderness along the physis in the presence of a
knee effusion
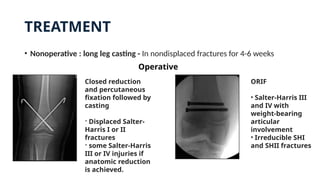
TREATMENT
• Nonoperative :long leg casting - In nondisplaced fractures for 4-6 weeks
Closed reduction
and percutaneous
fixation followed by
casting
- Displaced Salter-
Harris I or II
fractures
- some Salter-Harris
III or IV injuries if
anatomic reduction
is achieved.
ORIF
• Salter-Harris III
and IV with
weight-bearing
articular
involvement
• Irreducible SHI
and SHII fractures
Operative
26.
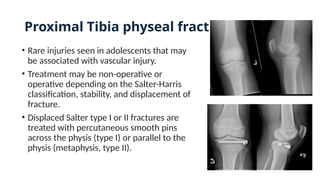
Proximal Tibia physealfracture
• Rare injuries seen in adolescents that may
be associated with vascular injury.
• Treatment may be non-operative or
operative depending on the Salter-Harris
classification, stability, and displacement of
fracture.
• Displaced Salter type I or II fractures are
treated with percutaneous smooth pins
across the physis (type I) or parallel to the
physis (metaphysis, type II).
27.
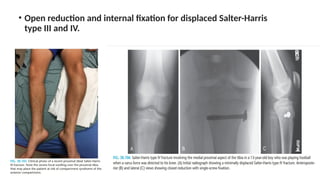
• Open reductionand internal fixation for displaced Salter-Harris
type III and IV.
28.
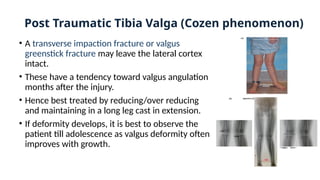
Post Traumatic TibiaValga (Cozen phenomenon)
• A transverse impaction fracture or valgus
greenstick fracture may leave the lateral cortex
intact.
• These have a tendency toward valgus angulation
months after the injury.
• Hence best treated by reducing/over reducing
and maintaining in a long leg cast in extension.
• If deformity develops, it is best to observe the
patient till adolescence as valgus deformity often
improves with growth.
29.
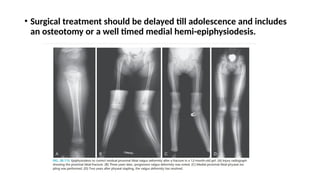
• Surgical treatmentshould be delayed till adolescence and includes
an osteotomy or a well timed medial hemi-epiphysiodesis.
30.
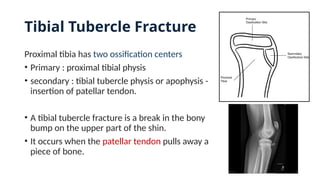
Tibial Tubercle Fracture
Proximaltibia has two ossification centers
• Primary : proximal tibial physis
• secondary : tibial tubercle physis or apophysis -
insertion of patellar tendon.
• A tibial tubercle fracture is a break in the bony
bump on the upper part of the shin.
• It occurs when the patellar tendon pulls away a
piece of bone.
31.
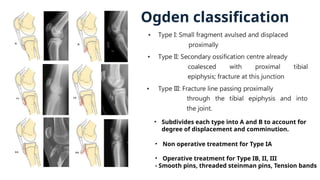
Ogden classification
• Subdivideseach type into A and B to account for
degree of displacement and comminution.
• Non operative treatment for Type IA
• Operative treatment for Type IB, II, III
- Smooth pins, threaded steinman pins, Tension bands
33.
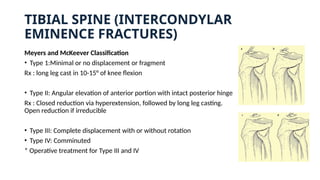
TIBIAL SPINE (INTERCONDYLAR
EMINENCEFRACTURES)
Meyers and McKeever Classification
• Type 1:Minimal or no displacement or fragment
Rx : long leg cast in 10-15° of knee flexion
• Type II: Angular elevation of anterior portion with intact posterior hinge
Rx : Closed reduction via hyperextension, followed by long leg casting.
Open reduction if irreducible
• Type III: Complete displacement with or without rotation
• Type IV: Comminuted
* Operative treatment for Type III and IV
34.
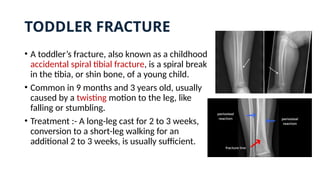
TODDLER FRACTURE
• Atoddler’s fracture, also known as a childhood
accidental spiral tibial fracture, is a spiral break
in the tibia, or shin bone, of a young child.
• Common in 9 months and 3 years old, usually
caused by a twisting motion to the leg, like
falling or stumbling.
• Treatment :- A long-leg cast for 2 to 3 weeks,
conversion to a short-leg walking for an
additional 2 to 3 weeks, is usually sufficient.
35.
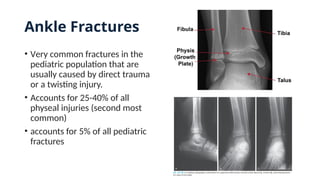
Ankle Fractures
• Verycommon fractures in the
pediatric population that are
usually caused by direct trauma
or a twisting injury.
• Accounts for 25-40% of all
physeal injuries (second most
common)
• accounts for 5% of all pediatric
fractures
36.
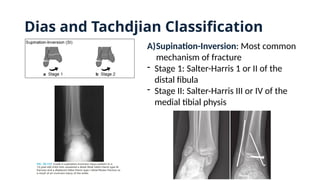
Dias and TachdjianClassification
A)Supination-Inversion: Most common
mechanism of fracture
- Stage 1: Salter-Harris 1 or II of the
distal fibula
- Stage II: Salter-Harris III or IV of the
medial tibial physis
37.
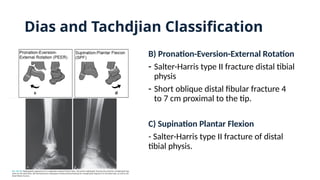
B) Pronation-Eversion-External Rotation
-Salter-Harris type II fracture distal tibial
physis
- Short oblique distal fibular fracture 4
to 7 cm proximal to the tip.
C) Supination Plantar Flexion
- Salter-Harris type II fracture of distal
tibial physis.
Dias and Tachdjian Classification
38.
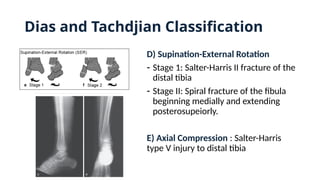
D) Supination-External Rotation
-Stage 1: Salter-Harris II fracture of the
distal tibia
- Stage II: Spiral fracture of the fibula
beginning medially and extending
posterosupeiorly.
E) Axial Compression : Salter-Harris
type V injury to distal tibia
Dias and Tachdjian Classification
39.
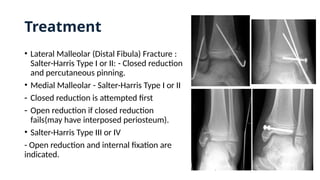
Treatment
• Lateral Malleolar(Distal Fibula) Fracture :
Salter-Harris Type I or II: - Closed reduction
and percutaneous pinning.
• Medial Malleolar - Salter-Harris Type I or II
- Closed reduction is attempted first
- Open reduction if closed reduction
fails(may have interposed periosteum).
• Salter-Harris Type III or IV
- Open reduction and internal fixation are
indicated.
40.
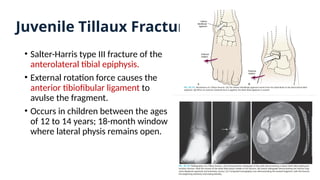
Juvenile Tillaux Fractures
•Salter-Harris type III fracture of the
anterolateral tibial epiphysis.
• External rotation force causes the
anterior tibiofibular ligament to
avulse the fragment.
• Occurs in children between the ages
of 12 to 14 years; 18-month window
where lateral physis remains open.
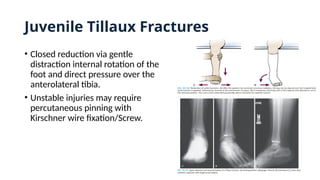
41.
• Closed reductionvia gentle
distraction internal rotation of the
foot and direct pressure over the
anterolateral tibia.
• Unstable injuries may require
percutaneous pinning with
Kirschner wire fixation/Screw.
Juvenile Tillaux Fractures
42.
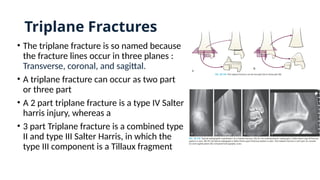
Triplane Fractures
• Thetriplane fracture is so named because
the fracture lines occur in three planes :
Transverse, coronal, and sagittal.
• A triplane fracture can occur as two part
or three part
• A 2 part triplane fracture is a type IV Salter
harris injury, whereas a
• 3 part Triplane fracture is a combined type
II and type III Salter Harris, in which the
type III component is a Tillaux fragment
43.
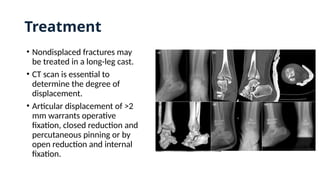
Treatment
• Nondisplaced fracturesmay
be treated in a long-leg cast.
• CT scan is essential to
determine the degree of
displacement.
• Articular displacement of >2
mm warrants operative
fixation, closed reduction and
percutaneous pinning or by
open reduction and internal
fixation.
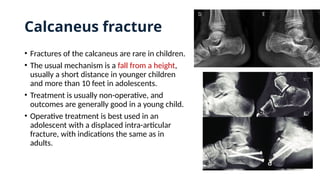
Calcaneus fracture
• Fracturesof the calcaneus are rare in children.
• The usual mechanism is a fall from a height,
usually a short distance in younger children
and more than 10 feet in adolescents.
• Treatment is usually non-operative, and
outcomes are generally good in a young child.
• Operative treatment is best used in an
adolescent with a displaced intra-articular
fracture, with indications the same as in
adults.































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






