

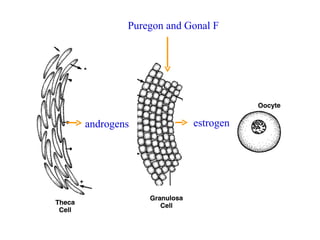
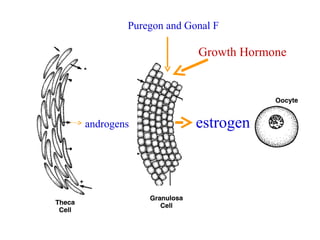
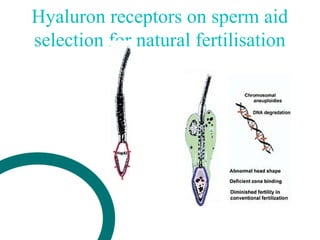
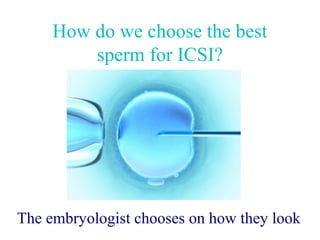
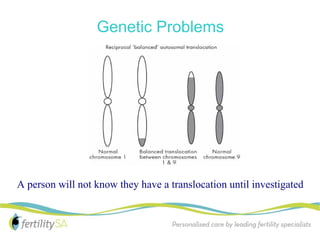
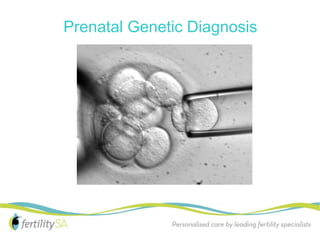

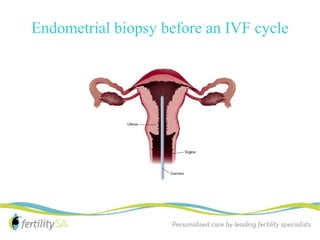

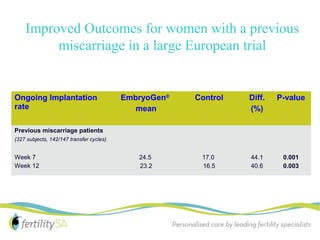
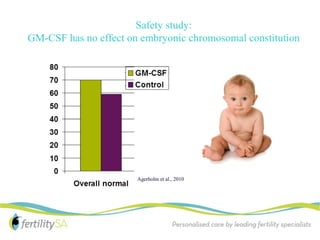
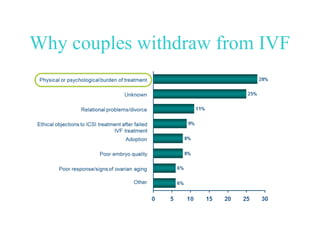


This document summarizes new directions in in vitro fertilization (IVF) being explored at FertilitySA to address common problems experienced by couples. These include using growth hormone to increase egg yield for those with low ovarian reserve, selecting sperm for ICSI based on hyaluron receptors, preimplantation genetic testing to identify genetic problems, endometrial biopsies to improve implantation, and culturing embryos in media containing GM-CSF to help with recurrent miscarriage. Ongoing trials are exploring the use of corifollitropin alfa to reduce injections and improve outcomes. The overall aim is to continue improving treatment through research and providing individualized care.




















































































