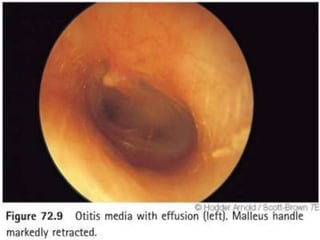
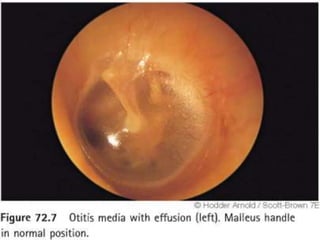
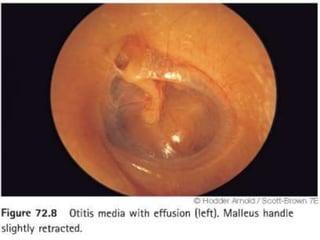
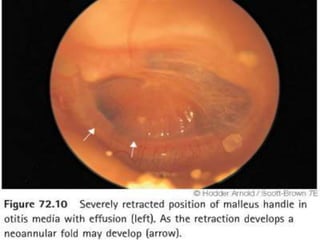
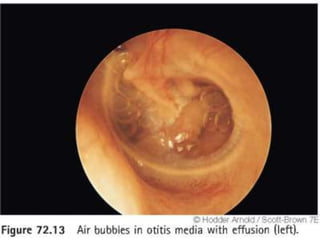
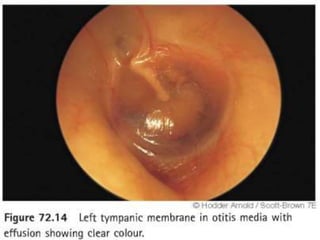
Otitis media with effusion (OME) in children requires different presentation, diagnosis, and management compared to adults, with significant prevalence following acute otitis media. The condition is characterized by fluid in the middle ear, influenced by factors such as eustachian tube dysfunction and infections, leading to hearing impairments. Current treatment options include observation, ventilation tubes, and adenoidectomy, with varying success in restoring hearing and managing symptoms.






































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







