The document provides information about otitis media, including:
- Otitis media is the most common illness-related medical visit for preschool children and the second most common diagnosis made by pediatricians.
- It mainly affects children from newborn to 7 years of age and occurs equally in males and females.
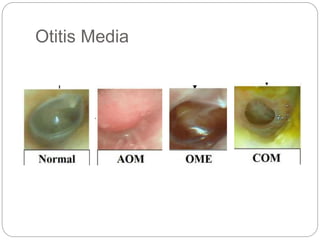
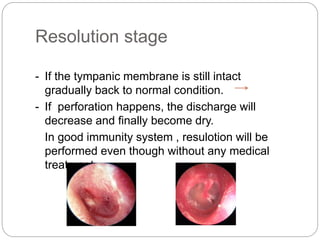
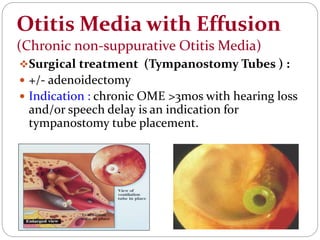
- Acute otitis media is a rapid onset middle ear infection lasting less than 3 months while chronic otitis media is a middle ear infection lasting more than 3 months characterized by recurrent discharge and perforation.
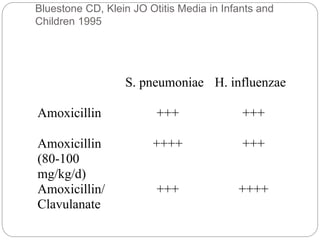
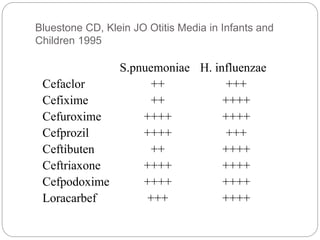
- Common causes are Streptococcus pneumoniae and Haemophilus influenzae bacteria. Risk factors include exposure to group childcare, smoke, and lack of breast






































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








