Download as PPSX, PPTX

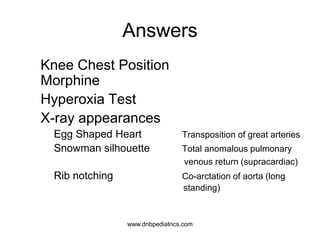
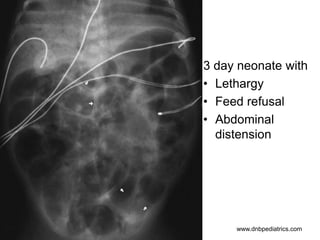



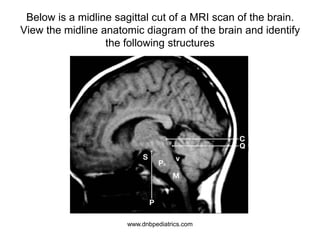
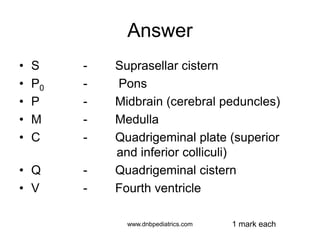

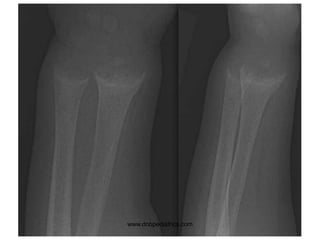






This document contains questions and answers related to pediatric imaging, cardiology, gastroenterology, hematology, neurology and other topics. It includes radiological images and questions about diagnoses, management, and embryology. The document is a study guide for the OSCE pediatrics exam covering various pediatric body systems and conditions assessed through imaging modalities like X-ray, CT and MRI.








































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














