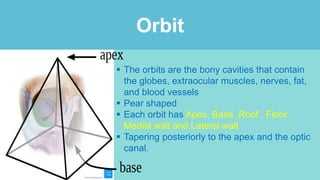
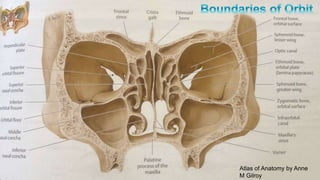
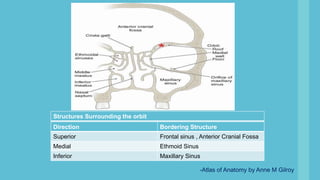
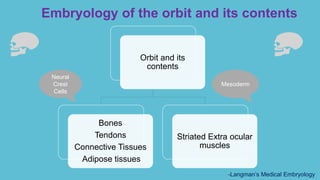
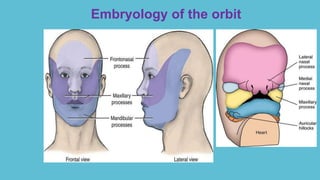
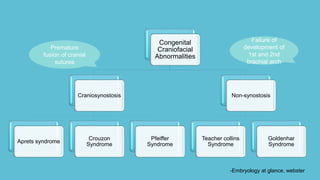
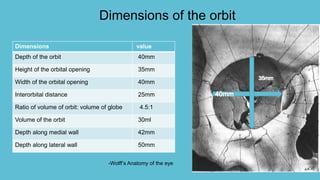
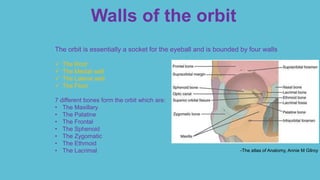
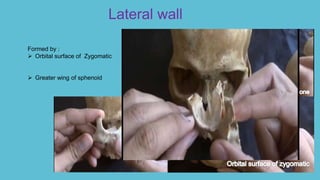
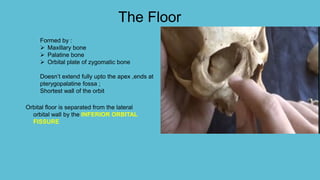
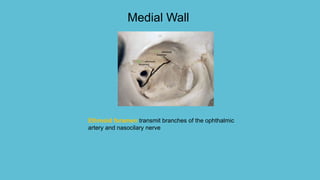
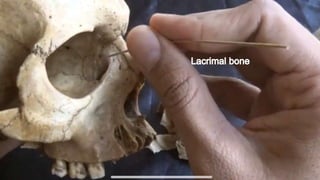
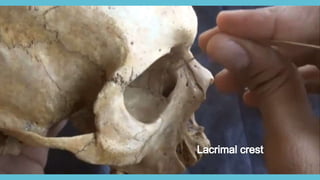
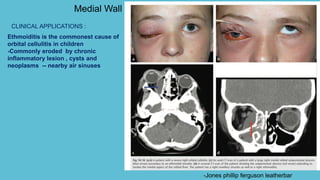
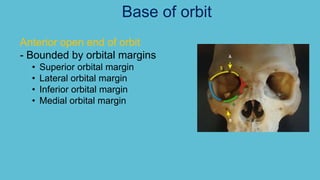
This document provides an overview of the anatomy of the orbit. It discusses the development, dimensions, walls and contents of the orbit. The orbits are pear shaped cavities containing the eyeballs and surrounding structures. They are bounded by the frontal, ethmoid, sphenoid, zygomatic and maxillary bones. The walls include the roof, medial, lateral and floor. The orbits taper posteriorly and contain the optic nerve, extraocular muscles, blood vessels and fat. Congenital abnormalities and clinical applications are also summarized.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







