Download as PDF, PPTX








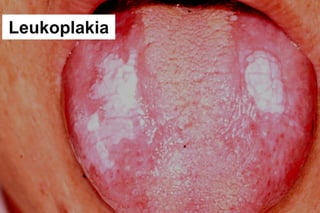


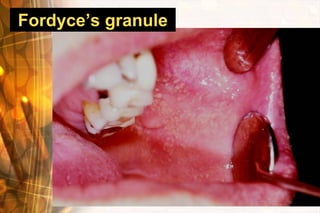

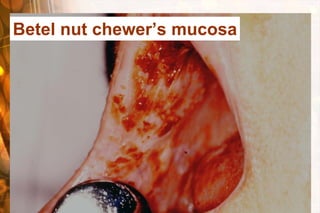







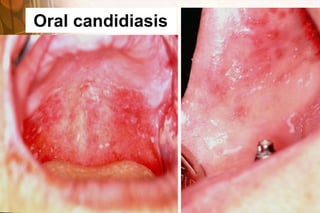












The document discusses common oral mucosal diseases. It begins by describing the structure and functions of oral mucosa. It then discusses methods of oral diagnosis including history taking, inspection, and special examinations. Finally, it covers common oral mucosal diseases such as traumatic ulcers, recurrent aphthous ulcers, tuberculosis, herpes simplex virus, lichen planus, candidiasis, oral cancer, and precancerous lesions. Risk factors for oral cancer include betel nut chewing which is common in Taiwan.




![Non infectivive stomatitis [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/non-infectivivestomatitisautosaved-180306071632-thumbnail.jpg?width=640&height=640&fit=bounds)







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










