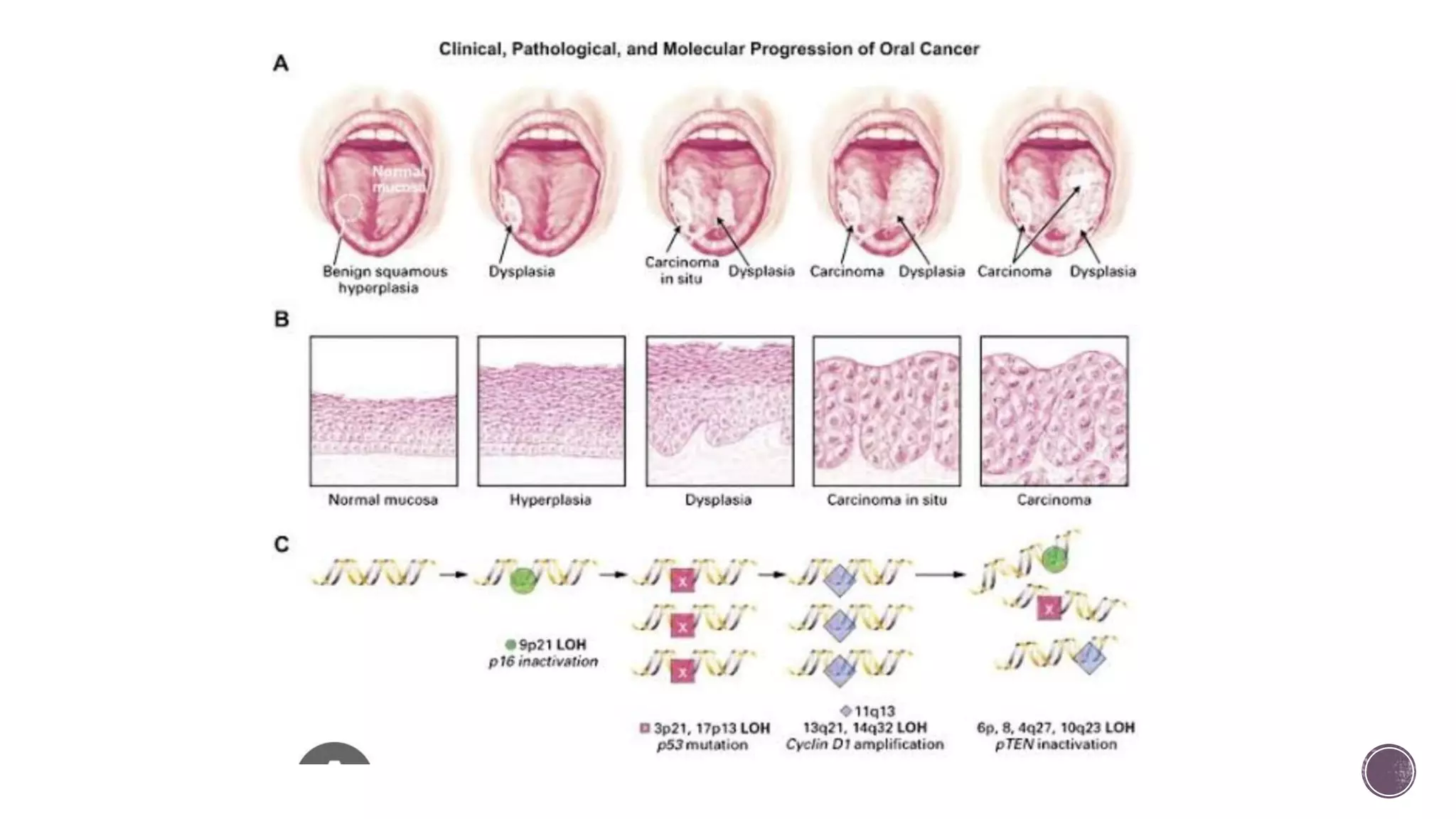
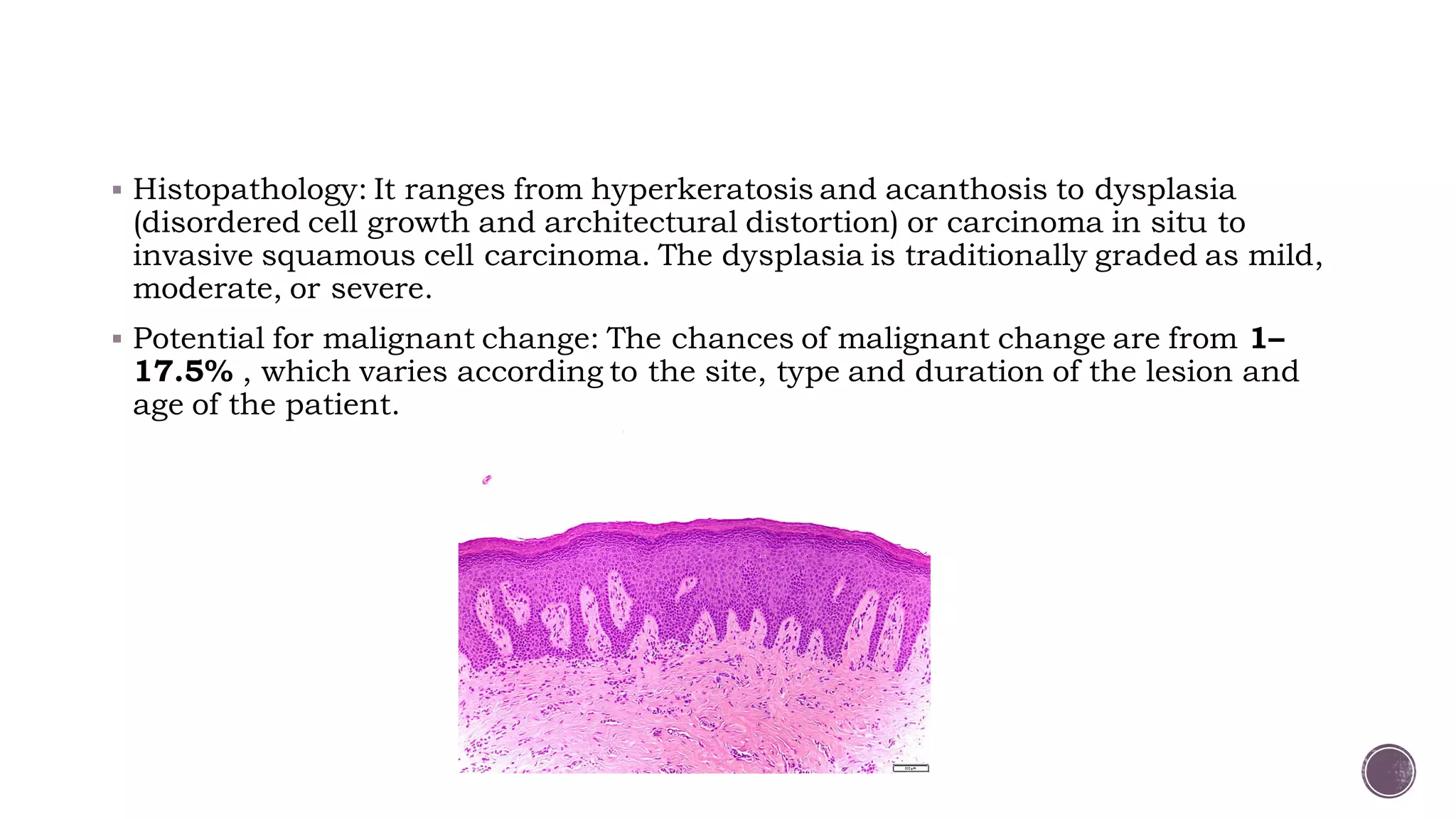
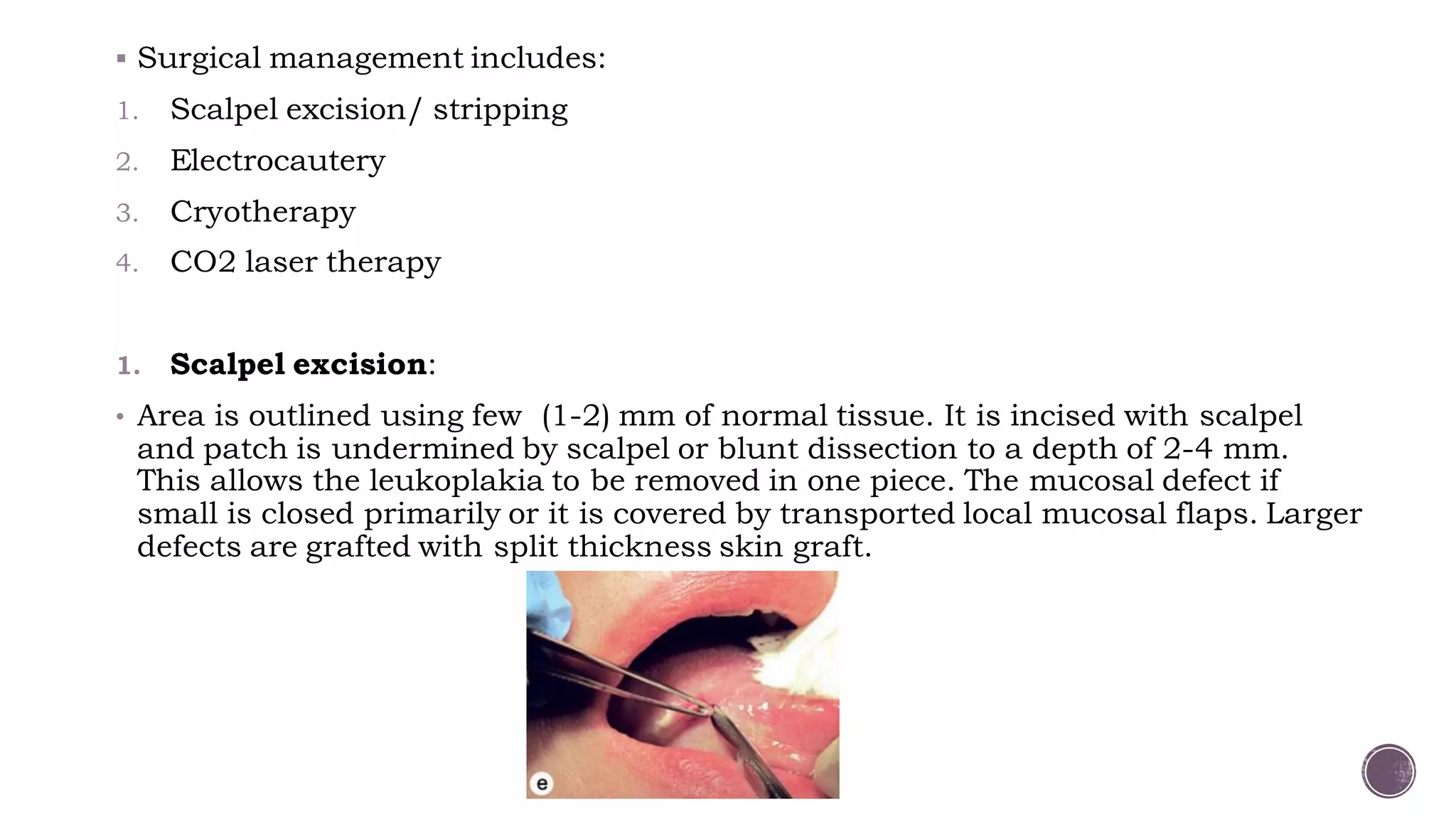
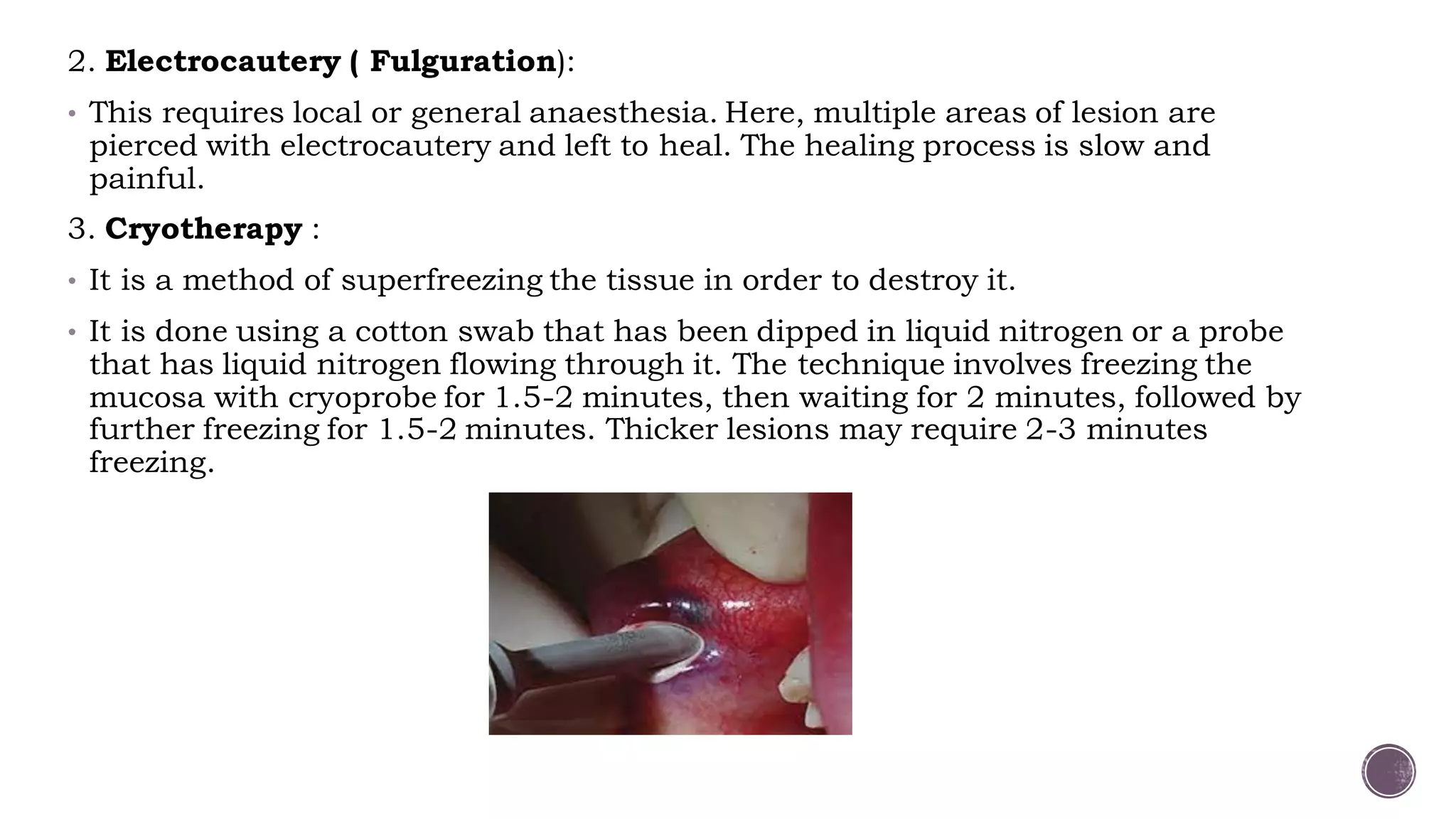
The document discusses various oral potentially malignant disorders, detailing their definitions, progression to oral cancer, risk factors, and management strategies. Key conditions covered include leukoplakia, erythroplakia, oral submucous fibrosis, and candidiasis, with insights on their clinical features, histopathology, and treatment options such as surgical and medical interventions. It emphasizes the importance of screening and early diagnosis to prevent malignant transformation of these lesions.