Downloaded 128 times






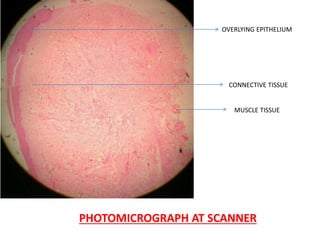
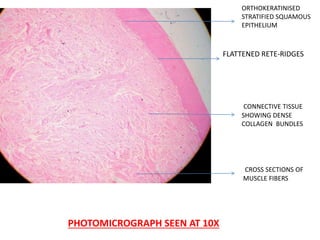
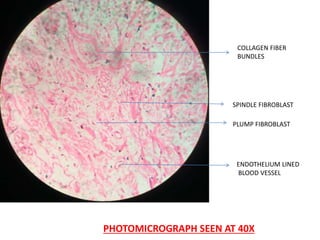














A 36-year-old female presented with a 3-year history of a painless mass in her left buccal mucosa. Examination found a 1cm red-white firm nodule. Biopsy revealed stratified squamous epithelium overlying dense collagen bundles and fibroblasts, consistent with fibroma. Fibromas are common benign tumors of the oral cavity occurring most often in the buccal mucosa of females in the third to fourth decade of life. Histopathological examination is needed to differentiate fibromas from other similar lesions and confirm the diagnosis.















































































