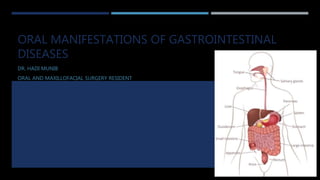
This document provides an overview of several gastrointestinal diseases and their potential oral manifestations. It discusses celiac disease, inflammatory bowel diseases like Crohn's disease and ulcerative colitis, orofacial granulomatosis, pyostomatitis vegetans and gangrenosum, and gastroesophageal reflux disease. For each condition, it describes the defining gastrointestinal symptoms and pathology, as well as common oral signs such as recurrent aphthous stomatitis, angular cheilitis, cobblestoning, and dental enamel defects. The document emphasizes that oral examination can help identify underlying bowel diseases, and management involves treating both the oral and gastrointestinal components of each condition.
Pericoronitis is inflammation of soft tissues surrounding the crown of partially erupted tooth including gingiva and dental follicle.
It can be acute, subacute or chronic.
The partially erupted or impacted mandibular third molar is the most common site of pericoronitis.
The lesion may be red swollen,suppurating along with the pain which may radiate to the surrounding tissues.
For more information book an appointment contact :
Dr.Rajat Sachdeva
Director & Mentor
Dr Sachdeva’s Dental Aesthetic And Implant Institute
I 101, Ashok Vihar Phase 1, Delhi- 110052
Contact us at
Phone : +919818894041,01142464041
Our Websites:
www.sachdevadentalcare.com
www.dentalimplantindia.co.in
www.dentalclinicindelhi.com
www.dentalcoursesdelhi.com
Google+ link: https://goo.gl/vqAmvr
Facebook link: https://goo.gl/tui98A
Youtube link: https://goo.gl/mk7jfm
Linkedin link: https://goo.gl/PrPgpB
Slideshare link : http://goo.gl/0HY6ep
Twitter Page : https://goo.gl/tohkcI
Instagram page : https://goo.gl/OOGVig
For Dentists : https://goo.gl/6t8DD5
A concise review on some conditions that cause epithelial erosion in the oral cavity.
This presentation covers some important lesions with clear diagrams for better comprehension.
Pericoronitis is inflammation of soft tissues surrounding the crown of partially erupted tooth including gingiva and dental follicle.
It can be acute, subacute or chronic.
The partially erupted or impacted mandibular third molar is the most common site of pericoronitis.
The lesion may be red swollen,suppurating along with the pain which may radiate to the surrounding tissues.
For more information book an appointment contact :
Dr.Rajat Sachdeva
Director & Mentor
Dr Sachdeva’s Dental Aesthetic And Implant Institute
I 101, Ashok Vihar Phase 1, Delhi- 110052
Contact us at
Phone : +919818894041,01142464041
Our Websites:
www.sachdevadentalcare.com
www.dentalimplantindia.co.in
www.dentalclinicindelhi.com
www.dentalcoursesdelhi.com
Google+ link: https://goo.gl/vqAmvr
Facebook link: https://goo.gl/tui98A
Youtube link: https://goo.gl/mk7jfm
Linkedin link: https://goo.gl/PrPgpB
Slideshare link : http://goo.gl/0HY6ep
Twitter Page : https://goo.gl/tohkcI
Instagram page : https://goo.gl/OOGVig
For Dentists : https://goo.gl/6t8DD5
A concise review on some conditions that cause epithelial erosion in the oral cavity.
This presentation covers some important lesions with clear diagrams for better comprehension.
Introduction
History
Epidemiology AIDS
CDC definition and classification of AIDS
Virus structure
Mode of transmission
Life cycle of HIV
Clinical features-WHO classification
Classification of oral lesions associated with HIV
Periodontal manifestations of HIV
Periodontal management of HIV infected patients
Diagnostic tests
Sterilization and precautions to be taken
Conclusion
burning mouth syndrome oral medicine
defined as burning, painful or itching sensation located in oral mucosa, the tongue is most affected part, followed by lips and palate.
BMS may be subclassifid into
“primary”
or idiopathic BMS for which a neuropathological cause is likely and cannot be attributed to any systemic or local cause
“secondary Oral and perioral burning sensation as a result of local or systemic factors or diseases is classifid as SBMS
Other names:
glossodynia, glossopyrosis, stomatodynia, stomatopyrosis, sore tongue and oral dysaesthesia
A burning or scalded sensation that most commonly affects your tongue, but may also
affect your lips, gums, palate, throat or whole mouth.
A sensation of dry mouth with increased thirst.
Taste changes to bitter or metallic taste.
To Book an Appointment:-
Dr. Rajat Sachdeva
+919818894041,01142464041
drrajatsachdeva@gmail.com
Follow us here:-
• Google+ link: https://goo.gl/vqAmvr
• Facebook link: https://goo.gl/tui98A
• Youtube link: https://goo.gl/mk7jfm
• Linkedin link: https://goo.gl/PrPgpB
• Slideshare link : http://goo.gl/0HY6ep
• Twitter Page : https://goo.gl/tohkcI
• Instagram page : https://goo.gl/OOGVig
Learn more:-
• www.sachdevadentalcare.com
• www.dentalclinicindelhi.com
• www.dentalimplantindia.co.in
• www.dentalcoursesdelhi.com
• www.facialaestheticsdelhi.com
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.
Introduction
History
Epidemiology AIDS
CDC definition and classification of AIDS
Virus structure
Mode of transmission
Life cycle of HIV
Clinical features-WHO classification
Classification of oral lesions associated with HIV
Periodontal manifestations of HIV
Periodontal management of HIV infected patients
Diagnostic tests
Sterilization and precautions to be taken
Conclusion
burning mouth syndrome oral medicine
defined as burning, painful or itching sensation located in oral mucosa, the tongue is most affected part, followed by lips and palate.
BMS may be subclassifid into
“primary”
or idiopathic BMS for which a neuropathological cause is likely and cannot be attributed to any systemic or local cause
“secondary Oral and perioral burning sensation as a result of local or systemic factors or diseases is classifid as SBMS
Other names:
glossodynia, glossopyrosis, stomatodynia, stomatopyrosis, sore tongue and oral dysaesthesia
A burning or scalded sensation that most commonly affects your tongue, but may also
affect your lips, gums, palate, throat or whole mouth.
A sensation of dry mouth with increased thirst.
Taste changes to bitter or metallic taste.
To Book an Appointment:-
Dr. Rajat Sachdeva
+919818894041,01142464041
drrajatsachdeva@gmail.com
Follow us here:-
• Google+ link: https://goo.gl/vqAmvr
• Facebook link: https://goo.gl/tui98A
• Youtube link: https://goo.gl/mk7jfm
• Linkedin link: https://goo.gl/PrPgpB
• Slideshare link : http://goo.gl/0HY6ep
• Twitter Page : https://goo.gl/tohkcI
• Instagram page : https://goo.gl/OOGVig
Learn more:-
• www.sachdevadentalcare.com
• www.dentalclinicindelhi.com
• www.dentalimplantindia.co.in
• www.dentalcoursesdelhi.com
• www.facialaestheticsdelhi.com
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.
LOWER GI HEMORRHAGE- PLAYLIST OF 6 VIDEOS
Dear Viewers,
Greetings from “Surgical Educator”.
I have made a playlist for Lower GI Hemorrhage which consists of six videos on various causes of Lower GI Hemorrhage. They are Introduction, diverticular disease, haemorrhoids, fissure-in-ano, colorectal carcinoma and inflammatory bowel disease. If you watch all these videos together you will become confident to tackle the clinical problem of Lower GI Hemorrhage. You can watch these videos in the following link: https://www.youtube.com/playlist…
Thank you for watching the videos.
This PowerPoint presentation demonstrate a useful review of Oral candidiosis, including its different types, clinical presentations, differential diagnosis, and treatment options.
A circumscribed ulceration of the GI mucosa occurring in areas exposed to acid and pepsin with a defect in the mucosa that extends through the
Muscularis mucosa into the
Submucosa or deeper.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
3. CELIAC DISEASES
Permanent intolerance to gliadin; the protein component of wheat. “Genetic”
Lifelong inflammatory condition of the gastrointestinal tract that affects the small intestine
Malabsorption due to morphological abnormalities in the small intestinal mucosa.
Reversible.
In adult coeliac disease, diarrhea, weight loss, and weakness are the classic signs and
symptoms.
“Celiac Sprue” Sprue: Dutch for Aphthous
4. CELIAC DISEASE
The incidence of biopsy-proven coeliac disease in the UK is 1 in 2000,
The incidence using markers as anti-endomysial antibodies actually approaches 1:300.
Approximately 5–10% of patients with coeliac disease have an affected first-degree relative.
Approximately 5–10% of people with Type I diabetes will also have coeliac disease.
Dermatitis herpetiformis is the classical non-gastrointestinal manifestation of coeliac disease.
Hematinic Deficiencies in Iron and Folate are likely to be present in Celiac Disease patients due to
malabsorption
5. DIAGNOSIS OF CELIAC DISEASE
Blood Tests; Full Blood Count and Hematinic assays, IgA anti-gliadin, IgA antireticulin, and IgA
endomysial autoantibodies.
Biopsy; Increased lymphocytic infiltration; Crypt hyperplasia occurs next then Villous Atrophy; Due to
Crypt Hyperplasia
Patients with positive blood tests but the biopsy is essentially normal are defined as having latent
coeliac disease.
7. ORAL MANIFESTATIONS OF CELIAC DISEASES
Recurrent Aphthous Stomatitis with coeliac disease in recent studies indicate it to be less than 5%.
Angular Cheilitis.
Dental enamel defects (hypoplasia) on the permanent teeth particularly lower incisors; indicates that
the celiac disease has been present at least in the first 2 years of life even though it might have been
clinically silent.
8. INFLAMMATORY BOWEL DISEASE
Lifelong conditions resulting from aberrant inflammation of the mucosal lining of the gastrointestinal
tract.
The two main categories are:
Crohn's disease, which may affect the gut anywhere
Ulcerative colitis, which is predominantly within the colon.
Oral involvement has been recognized in patients suffering from both Crohn's disease and to a lesser
extent, ulcerative colitis.
Oral lesions may precede or accompany gastrointestinal disease and can be the only site of involvement.
9. CROHN’S DISEASE
Was described as “Regional Ileitis”.
Mucosal inflammation and ulceration, obstructive edema [Lymph Node Hyperplasia] and the production
of granulomatous lesions.
The clinical progression of the disease is very variable with inactive phases.
10. AGGRESSIVE STAGES OF CROHN’S DISEASE
Abdominal pain
Diarrhea
Malaise
The production of fistulae.
Arthropathies
Skin granulomas
11. TREATMENT OF CROHN’S DISEASE
The aetiology of the disease is not known.
Treatment is medical; using steroids, azathioprine (and other immunosuppressive agents) or amino-
salicylates
Dietary treatment strategies; favored in children.
Replacement therapy to correct malabsorption.
Surgery.
12. OROFACIAL GRANULOMATOSIS
The term ‘orofacial granulomatosis’ (OFG) was introduced to encompass these disorders and to describe
a clinical syndrome presenting with swelling of the face, lips, or oral tissues with histological evidence of
noncaseating granulomatous inflammation.
Oral Crohn's disease
Oral sarcoid
Melkersson–Rosenthal syndrome
Mieschener's Cheilitis granulomatosa (granulomatous Cheilitis).
13. CLINICAL FEATURES OF OFG AND CROHN’S
The most common feature is: Orofacial swelling, particularly involving the lips
Painless, firm ‘rubbery’ consistency; and can involve both lips with varying severities.
The floor of the mouth, periorbital and chin regions can be occasionally involved.
The buccal mucosa is thickened and folded, characteristic ‘COBBLESTONE’ appearance.
Lip fissures and Angular Cheilitis.
History of recurrent or persistent swelling of the submandibular lymph nodes. There may also be
persistent erythema and scaling of the perioral tissues. Mucosal tags may be present, particularly in the
retromolar regions.
14. CLINICAL FEATURES OF OFG AND CROHN’S
RAS and NON-RAS ulcers
Persistent linear ulcers occur in the buccal and labial sulci at the base of hyperplastic tissue, can be painful,
particularly when eating.
The gingivae may appear hyperplastic and edematous and usually has a “full thickness pattern” – GM to
Non-Keratin.
18. HISTOLOGY OF OFG
Noncaseating and epithelioid granulomas, with or without multinucleated giant cells, are seen in
90% of the cases.
Granulomas are not always present and their absence does not exclude the clinical diagnosis of
OFG.
19. OFG AS A PREDICTOR TO CROHN’S?
The interrelationship between oral Crohn's disease and OFG is a matter for debate.
In one study, 10% of 60 OFG patients had definite evidence of Crohn's disease affecting the intestine.
Another study demonstrated asymptomatic intestinal involvement in 37% who presented solely with
features of OFG.
The prevalence of asymptomatic intestinal disease in patients with OFG has been reported as between
10 and 50% in various series.
20. AETIOLOGY OF OROFACIAL GRANULOMATOSIS
The aetiology of OFG unrelated to systemic disease remains unclear.
Allergy, Infections, and hereditary causes have all been implicated, together with infectious agents such as
Saccharomyces cerevisiae, Mycobacterium Para-tuberculosis , and ‘Campylobacter-like’ bacteria.
Clinical atopy is more prevalent in OFG.
It remains unknown whether sensitivity to food additives is the primary factor for some patients with OFG or a
secondary aggravating factor to an underlying process.
21. DIAGNOSIS OF OROFACIAL GRANULOMATOSIS
Hematological investigations
Biochemical investigations, including inflammatory markers
Estimation of the serum Angiotensin Converting Enzyme (ACE)
Chest X-Ray
Biopsy [deeper beyond the superficial tissue].
Esophago-Gastro-Duodenoscopy
Ileo-Colonoscopy
Small bowel radiographs
22. MANAGEMENT OF OROFACIAL GRANULOMATOSIS
Treatment of OFG is unsatisfactory and response to drug-therapy is disappointing.
Lip-swelling can cause considerable embarrassment.
Short courses of systemic steroids can be effective at reducing the swelling
Long-term systemic steroids are contraindicated, particularly in children.
Intralesional steroids.
A large number of systemic drugs have been tried with mixed success [Azathioprine, Clofazimine,
Hydroxychloroquine, Danazol, cyclosporine, sulazosulfapyridine, thalidomide, and antimicrobials ]
Topical steroids and antiseptic and analgesic mouthwashes for managing the oral ulceration.
Angular Cheilitis and lip fissures frequently become secondarily infected can be improved by the
application of an antifungal cream
23. ULCERATIVE COLITIS
Young adult life
Inflammatory changes in the colonic mucosa and submucosa lead to widespread ulceration.
May be complicated by hemorrhage, perforation, and, occasionally malignancy.
Pain, diarrhea, and generalized abdominal discomfort are the predominant symptoms.
‘Diseases of civilization’.
The treatment of ulcerative colitis is by the use of sulfasalazine and steroids, used either locally or
systemically.
Surgery may be necessary if medical treatment fails.
Ulcerative colitis only affects the large bowel.
24.
25. PYOSTOMATITIS VEGETANS
Rare oral Disorder and a highly specific marker for IBD.
The bowel symptoms often precede oral involvement by several months or years.
Male: Female ratio = 3:1 and affects all ages.
It is the oral equivalent of pyoderma vegetans.
26. PYOSTOMATITIS VEGETANS
Miliary abscesses and pustular lesions affecting the oral mucosa and gingiva
Gingivae become thickened, erythematous, and may exhibit vegetations or ‘cobblestoning’.
‘Snail-track’ ulcers.
The oral lesions predominantly affect the labial, buccal mucosa and the labial gingiva can
affect the hard and soft palate, vestibule, and tonsillar region.
The histological features are often characteristic, although not pathognomonic, showing
intraepithelial and sub-epithelial microabscesses containing large numbers of eosinophils.
27. TREATMENT OF PYOSTOMATITIS VEGETANS
Topical steroid therapy has been successful for the treatment.
Systemic treatment, with or without azathioprine or sulfamethoxypyridazine is required.
Management of the associated IBD may also result in improvement of the oral lesions.
It has been suggested that all patients should be investigated for bowel disease.
31. PYOSTOMATITIS GANGRENOSUM
Other forms of stomatitis have been reportedly associated with IBD and
include irregular, deep, foul-smelling ulcers of varying size, with rolled
margins and a greyish, fibrinous base.
32. GASTRO- ESOPHAGEAL REFLUX DISEASE (GERD)
Healthy individuals experience GERD after a meal and this is due to the relaxation of the lower
esophageal sphincter.
In patients with GERD, there is increased frequency and duration of reflux and the esophageal
mucosa is damaged by regurgitation of gastric contents.
Reflux esophagitis, ulceration, stricture, or epithelial metaplasia (Barrett's oesophagus).
33. CLINICAL FEATURES OF GERD
Heart-burn
Epigastric pain and regurgitation.
The ‘silent refluxers’ have no symptoms.
Dental erosion particularly of the palatal aspects of the teeth.
Patients who regularly chew antacid preparations may have a high sugar content that can
predispose to caries.
Orofacial manifestations of iron deficiency.
34. TREATMENT OF GERD
Simple antacids or covering agents
H2 receptor blockers (cimetidine) that inhibit gastric acid secretion.
Proton-pump inhibitors (omeprazole) that inhibit acid production.
Surgery is rarely indicated. [Periodic Dilation]