Download as PDF, PPTX

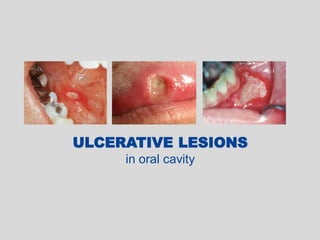














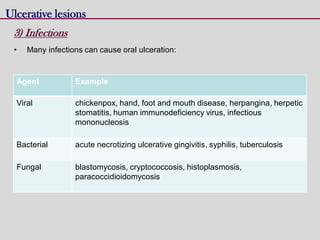


This document discusses various types of ulcerative lesions that can occur in the oral cavity. It defines an ulcer as a local defect or excavation of the surface of an organ or tissue. The main causes of oral ulceration discussed are local trauma, aphthous ulcers, infections such as herpes, drugs, malignancies, and systemic diseases. Physical trauma is a common local cause of ulcers from factors like sharp teeth or dental appliances. Ulcerative lesions can also be caused by chemical or thermal burns in the mouth.



































































