Download to read offline


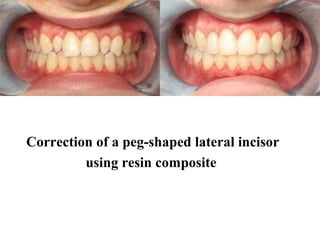





The document discusses various types of dental composites used for restorations, including packable, flowable, and low-shrinking silorane composites, detailing their properties, advantages, and disadvantages. It emphasizes the importance of resin composites for aesthetic enhancements and their application in different cavity preparations while highlighting the need for proper bonding and isolation techniques during procedures. Additionally, the document covers contraindications for use and outlines the steps required for resin composite restoration application.






















































































