
Downloaded 165 times
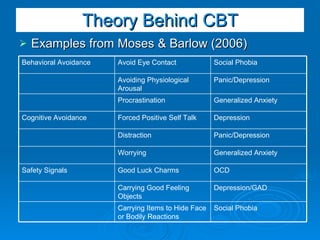
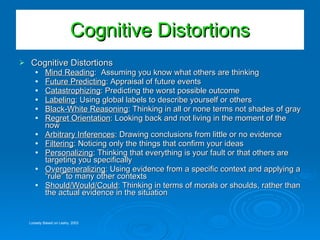
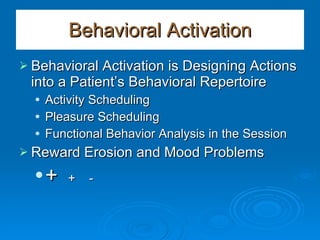
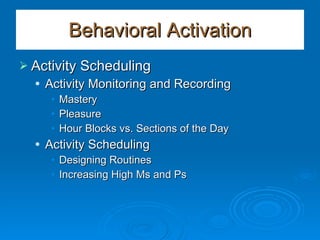
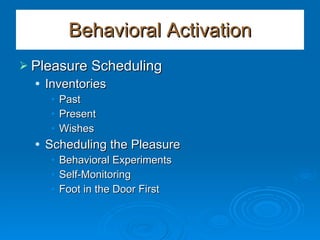

The document provides an overview of cognitive-behavioral therapy (CBT) strategies and techniques. It discusses Barlow's model of emotional disorders and how CBT addresses emotional regulation, cognitive appraisals, emotionally-driven behaviors, and avoidance. The basic CBT model examines psychopathology through a bio-psycho-social lens and addresses maladaptive cognitions and behaviors. Common CBT techniques include identifying cognitive distortions, challenging thoughts through questioning and experimentation, and behavioral activation methods like activity scheduling.



























































![Anxiety disorders unit intervention[2]](https://cdn.slidesharecdn.com/ss_thumbnails/anxietydisordersunitintervention2-111028091300-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







