Downloaded 274 times


























![References
• Beckmann, C., Herbert, W., Laube, D., Ling, F., Smith, R., & American
College of Obstetricians Gynecologists. (2014). Obstetrics and
gynecology (7th ed.).
• http://www.stanfordchildrens.org/en/topic/default?id=amniocentesis
-90-P02429
• Callahan, T., & Caughey, A. (2007). Blueprints obstetrics & gynecology
(4th ed. / Tamara L. Callahan, Aaron B. Caughey. ed., Blueprints).
Philadelphia ; London: Lippincott Williams & Wilkins.
• Cunningham, F., & Williams, J. (2014). Williams obstetrics. (24th ed. /
[edited by] F. Gary Cunningham et al. ed.). New York ; London:
McGraw-Hill Medical.](https://image.slidesharecdn.com/03-160613133816/75/Oligohydramnios-and-IUGR-30-2048.jpg)
![References
• Beckmann, C., Herbert, W., Laube, D., Ling, F., Smith, R., & American College of
Obstetricians Gynecologists. (2014). Obstetrics and gynecology (7th ed.).
• https://ghr.nlm.nih.gov/condition/vacterl-association
• https://www.uptodate.com/contents/placental-abruption-clinical-features-and-
diagnosis?source=machineLearning&search=abruptio+placenta&selectedTitle=1~
150§ionRank=1&anchor=H4#H4
• Cunningham, F., & Williams, J. (2014). Williams obstetrics. (24th ed. / [edited by]
F. Gary Cunningham et al. ed.). New York ; London: McGraw-Hill Medical.
• https://www.uptodate.com/contents/oligohydramnios?source=search_result&se
arch=oligohydramnios&selectedTitle=1~150
• Callahan, T., & Caughey, A. (2007). Blueprints obstetrics & gynecology (4th ed. /
Tamara L. Callahan, Aaron B. Caughey. ed., Blueprints). Philadelphia ; London:
Lippincott Williams & Wilkins.](https://image.slidesharecdn.com/03-160613133816/75/Oligohydramnios-and-IUGR-31-2048.jpg)


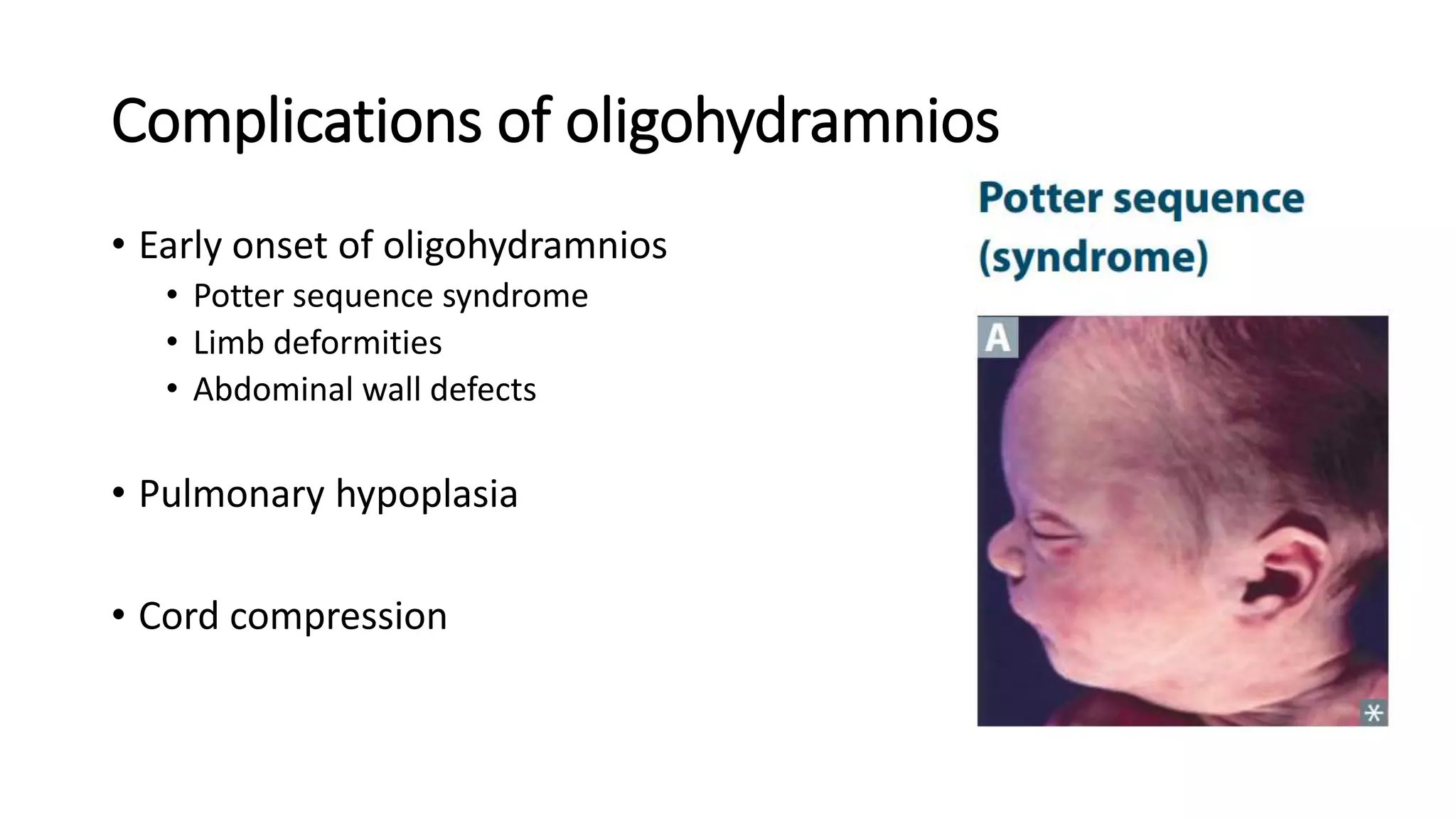
This document discusses oligohydramnios and intrauterine growth restriction (IUGR). It begins by explaining the functions of amniotic fluid, including allowing fetal movement, swallowing, breathing, and preventing umbilical cord compression. It then defines oligohydramnios as a decreased amniotic fluid index or single deepest pocket, and notes its association with uterine size smaller than gestational age and IUGR. Complications of oligohydramnios include limb deformities and pulmonary hypoplasia. The document also discusses evaluating and managing cases of oligohydramnios and IUGR, including admission, testing, monitoring fetal distress, and indications for delivery.