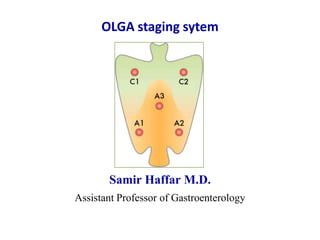
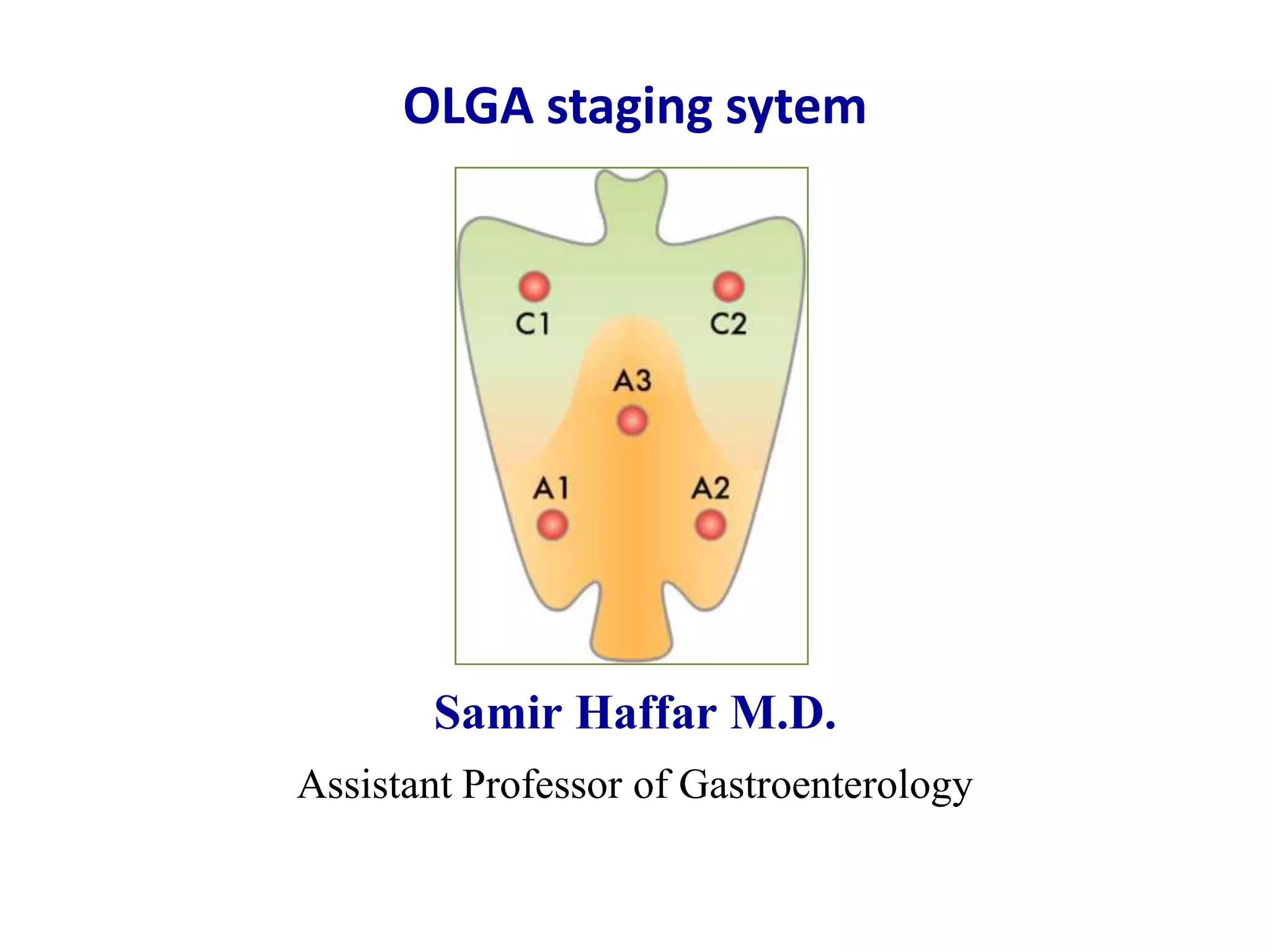
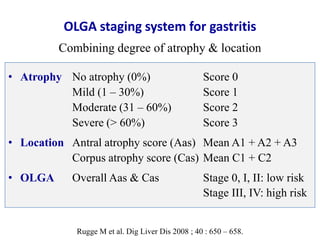
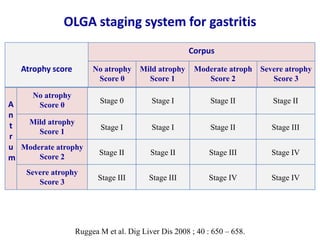
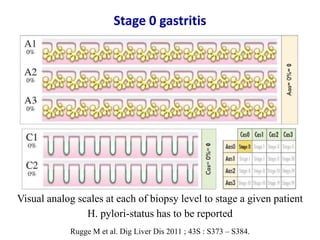
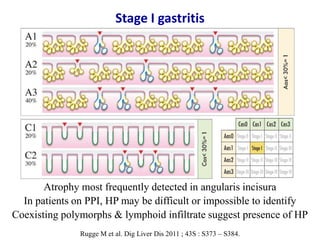
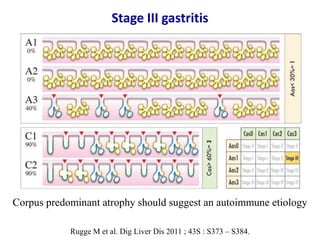
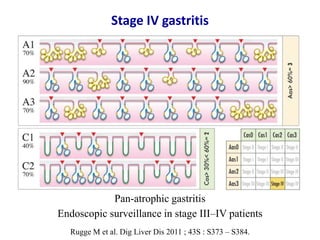
This document summarizes the OLGA staging system for classifying and assessing the risk of gastric cancer from gastritis. The OLGA system stages gastritis from Stage 0 to Stage IV based on the degree and location of gastric atrophy identified on biopsy. Stages 0-II are considered low risk for gastric cancer while Stages III-IV are high risk. The staging is done by combining an antrum atrophy score and corpus atrophy score assessed from biopsies of the gastric antrum and corpus according to a standardized sampling protocol.