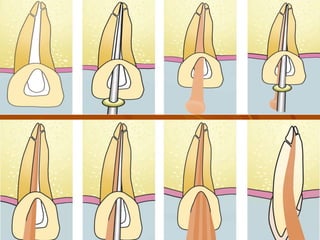
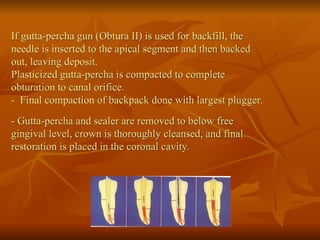
Obduration is the three-dimensional filling of the root canal system, historically using various materials, with gutta-percha becoming popular in the 19th century. The primary objectives include achieving a fluid impervious seal and addressing any canal irregularities, with materials classified by types and ideal properties outlined. Techniques for obturation include cold lateral compaction and warm compaction methods, both crucial for the success of endodontic treatment, highlighting that proper obturation significantly impacts the treatment's outcome.





![GUTTA PERCHA BASED SEALERS
CHLOROPERCHA
[chloroform + gutta percha]
Not adhesive
Increased shrinkage
Decreased radiopacity
Chloroform – potential carcinogen
EUCAPERCHA
eucalyptol
gutta percha
CALLAHAN-
JOHNSTON TECHNIQUE
[DIFFUSION TECHNIQUE]
Chloroform + rosin
gutta percha
KLOROPERKA N- Ø
chloroform + resin + zinc oxide
gutta percha](https://image.slidesharecdn.com/obturationtechniques-240915182709-90e99e12/85/OBTURATION-TECHNIQUES-methods-types-and-uses-32-320.jpg)