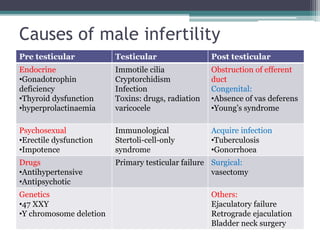
This document discusses infertility, including its definition, causes, investigations, and treatments. It defines primary and secondary infertility and notes that most couples conceive within 1-2 years. Major causes of male infertility include varicocele, infections, genetic issues, and immunological factors. For females, common causes are ovulatory disorders, tubal damage from infections, uterine factors like fibroids, and endometriosis. Investigations involve medical histories, physical exams, and lab tests. Treatments include lifestyle changes, medications to induce ovulation, surgery to repair tubes or treat endometriosis, and assisted reproductive technologies like IVF for severe cases. The prognosis is that 30-40% of couples conceive within 2 years with treatments.