1. ANTENATAL CARE
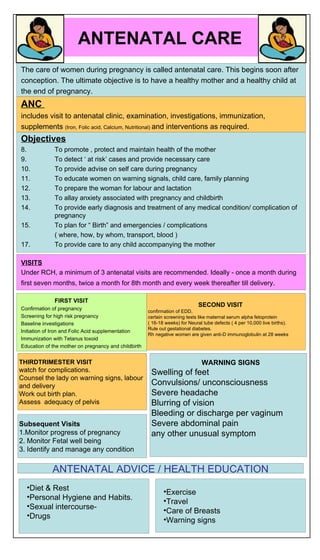
The care of women during pregnancy is called antenatal care. This begins soon after
conception. The ultimate objective is to have a healthy mother and a healthy child at
the end of pregnancy.
ANC
includes visit to antenatal clinic, examination, investigations, immunization,
supplements (Iron, Folic acid, Calcium, Nutritional) and interventions as required.
Objectives
8. To promote , protect and maintain health of the mother
9. To detect ‘ at risk’ cases and provide necessary care
10. To provide advise on self care during pregnancy
11. To educate women on warning signals, child care, family planning
12. To prepare the woman for labour and lactation
13. To allay anxiety associated with pregnancy and childbirth
14. To provide early diagnosis and treatment of any medical condition/ complication of
pregnancy
15. To plan for “ Birth” and emergencies / complications
( where, how, by whom, transport, blood )
17. To provide care to any child accompanying the mother
VISITS
Under RCH, a minimum of 3 antenatal visits are recommended. Ideally - once a month during
first seven months, twice a month for 8th month and every week thereafter till delivery.
FIRST VISIT
SECOND VISIT
Confirmation of pregnancy confirmation of EDD,
Screening for high risk pregnancy certain screening tests like maternal serum alpha fetoprotein
Baseline investigations ( 16-18 weeks) for Neural tube defects ( 4 per 10,000 live births).
Rule out gestational diabetes.
Initiation of Iron and Folic Acid supplementation
Rh negative women are given anti-D immunoglobulin at 28 weeks
Immunization with Tetanus toxoid
Education of the mother on pregnancy and childbirth
THIRDTRIMESTER VISIT WARNING SIGNS
watch for complications. Swelling of feet
Counsel the lady on warning signs, labour
and delivery Convulsions/ unconsciousness
Work out birth plan. Severe headache
Assess adequacy of pelvis Blurring of vision
Bleeding or discharge per vaginum
Subsequent Visits Severe abdominal pain
1.Monitor progress of pregnancy any other unusual symptom
2. Monitor Fetal well being
3. Identify and manage any condition
ANTENATAL ADVICE / HEALTH EDUCATION
•Diet & Rest
•Exercise
•Personal Hygiene and Habits.
•Travel
•Sexual intercourse-
•Care of Breasts
•Drugs
•Warning signs
2. INTRANATAL CARE
OBJECTIVES
• Thorough ASEPSIS (“The Five Cleans” - clean hands, surface, blade, cord, tie)
• MINIMUM INJURY to mother and child
• To deal with any COMPLICATIONS
• Care of the NEWBORN
Institutional delivery is a must if there is
2. Mild pre-eclampsia
3. PPH in the previous pregnancy
4. More than 5 previous births or a primi
5. Previous assisted delivery
6. Maternal age less than 16 years
7. H/o third-degree tear in the previous pregnancy
8. Severe anaemia
9. Severe pre-eclampsia/eclampsia
10. Antepartum Hemorrhage
11. Transverse fetal lie or any other Malpresentation
12. Caesarean section in the previous pregnancy
13. Multiple pregnancies
14. Premature or pre-labour rupture of membranes (PROM)
15. Medical illnesses such as diabetes mellitus, heart disease, asthma, etc.
16. Pregnancy in women who are HIV positive
DELIVERY AT REFERRAL CENTRE
DELIVERY AT PHC IF • Prior delivery by caesarean.
■ First birth. • Age less than 14 years.
■ Last baby born dead or died in first day. • Transverse lie or other obvious malpresentation
■ Age less than 16 years. within one month of expected delivery.
■ More than six previous births. • Obvious multiple pregnancy.
■ Prior delivery with heavy bleeding. • Tubal ligation or IUD desired immediately
■ Prior delivery with convulsions. after delivery.
■ Prior delivery by forceps or vacuum. • Documented third degree tear.
■ HIV-positive woman. • History of or current vaginal bleeding or other
complication during this pregnancy.
Role of Birth Attendant/ Midwife
• Explain all the procedures
• Praise the woman, encourage her and reassure her that things are going well.
• Encourage the woman to bathe or wash herself and her genitals at the onset of labour.
• Always wash your hands with soap and water before examining the woman
• Ensure cleanliness of the birthing area.
• Enema should be given only when needed.
• Encourage the woman to empty her bladder frequently.
• Non-pharmacological methods of relieving pain during labour
RECORD OF-
Contractions, their intensity, frequency and duration are recorded.
Cervical dilatation and effacement are recorded.
FHS, amniotic fluid, vitals of the mother, fluid balance, drugs administered etc.
Readily available tool for decision making.
Advantages:
1. reduced prolonged labours and instrumental deliveries;
2. higher APGAR scores and
3. lower perinatal mortality.
WHO modified Partograph- No latent phase
3. POSTNATAL CARE
Puerperium begins after the placenta is expelled and lasts for 6-8 weeks
The Puerperium is characterized by –
1. Return of generative organs to pre-gravid state,
2. initiation of lactation and
3. Recovery from physical, hormonal and emotional experience of the parturition.
POSTNATAL CARE
postpartum care is aimed at achieving a Puerperium which is free of any complications and to ensure a healthy newb
ECTIVES
estoration of mother to optimum health
prevent complications of puerperium
ovide basic postpartum care and services to mother and child
otivate, educate and provide family planning services
check adequacy of breast feeding
Monitor the following HELP IS NECESSARY IF-
- every 10 minutes for the first 30 minutes, • Bleeding increases.
- then every 15 minutes for the next 30 minutes, • Feels dizzy.
- and then every 30 minutes for the next three hours: • Severe headache.
BP, pulse, temperature, vaginal bleeding, uterus • Visual disturbance.
Ask the birth companion to stay with the mother. • Epigastric distress.
Do not leave the mother and the newborn alone. • Breathlessness.
• Woman complains of increased abd/ perineal pain
VISITS
day 7th, or ask the ANM in charge of that area to pay a home visit during this period.
hin 7-10 days after delivery. Either ask the ANM of that area to pay a visit to the woman and her baby, or ask the wom
n of uterus is complete.
ter every 2-3 months till the end of one year.
COMPLICATIONS Advise the woman to visit the
Advise the woman to go to
•Puerperal sepsis PHC as soon as possible if-
an FRU WITHOUT WAITING. (i) Fever
•Urinary tract infections (i)Excessive vaginal bleeding, (ii) Abdominal pain
•Breast infections (iii) The woman feels ill
(ii)Convulsions (iv) Swollen, red or tender breasts
•Venous thrombosis
•Pulmonary thromboembolism (iii)Fast or difficult breathing or sore nipples
(v) Dribbling of urine or painful
•Puerperal haemorrhage (iv)Fever and weakness micturition
•Incontinence of urine (v)Severe abdominal pain (vi) Pain in the perineum, or pus
draining from the perineal area
•Psychiatric disorders (vii) Foul-smelling lochia.
All India Hospital Post partum Program
egun in 1969 with 54 participating hospitals,
With a view to provide maternal, child health and family welfare services in semi-urban/ rural areas,
he training of medical students and graduates in the techniques of birth control is an important aspect of the program
he major purpose of the program is to convince maternity and abortion patients to adopt birth control practices
ural areas are reached through the medical colleges and attached hospitals which have responsibility for the area.
ducational programs
ost Partum PAP Smear Test Facility Programme