Downloaded 77 times

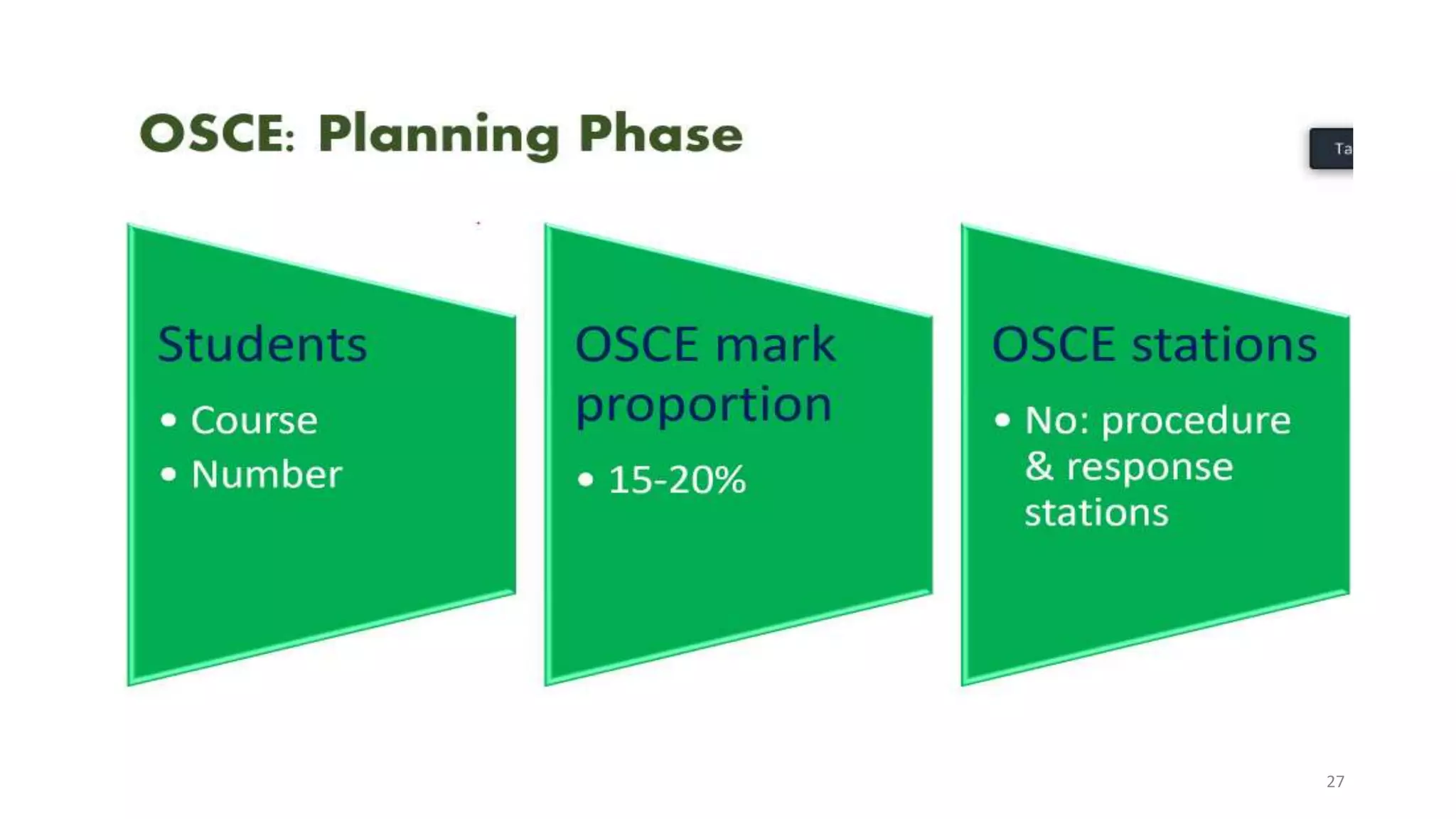
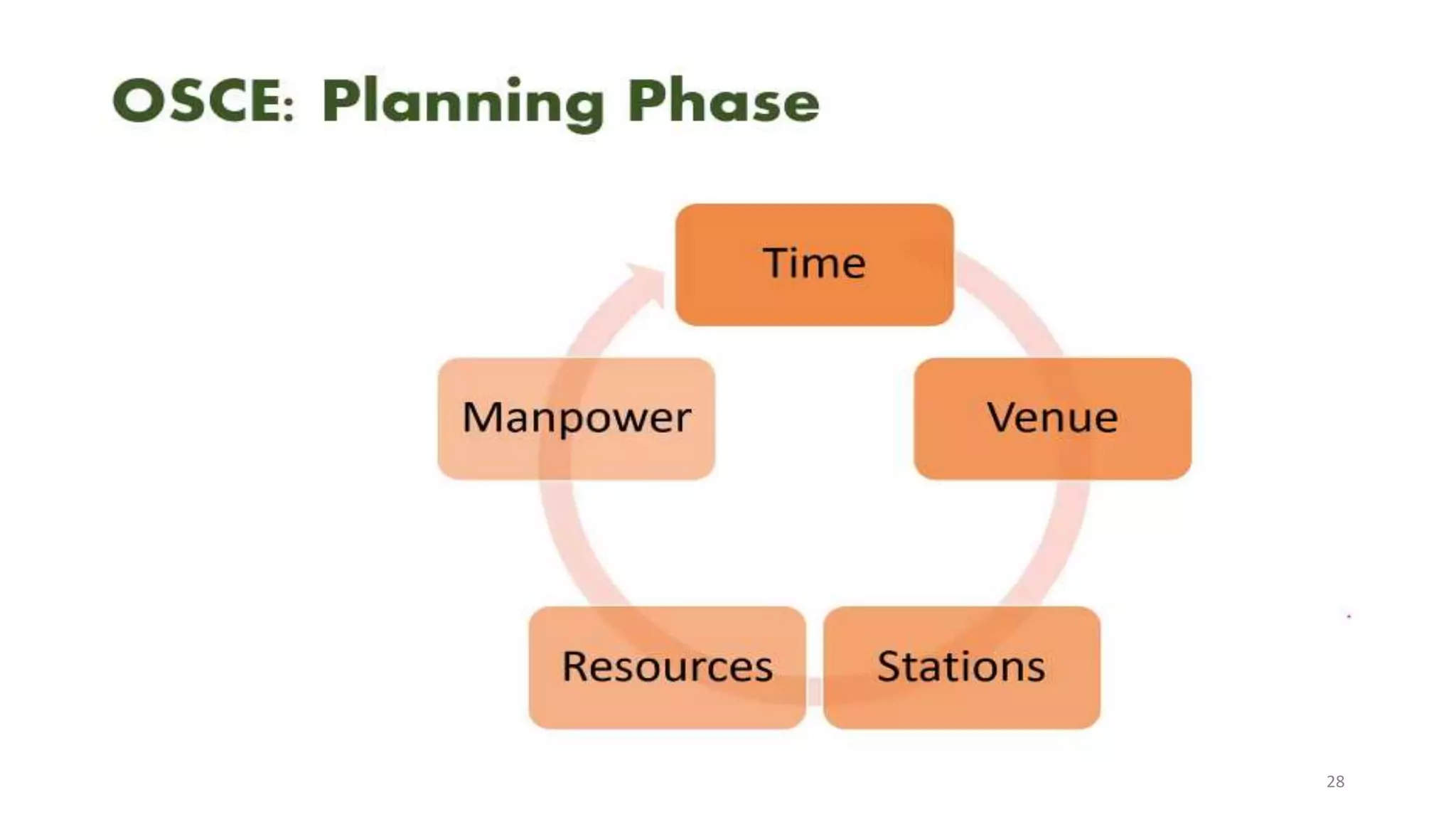



The document discusses Objective Structured Clinical Examination (OSCE) which is used to assess clinical competence of students. It involves students demonstrating skills at various stations using standardized patients. The document outlines the history, purpose, planning and administration of OSCEs. It notes the method was developed in the 1970s and is now widely used globally to evaluate skills like history taking, physical exams, and procedures in an objective structured manner.