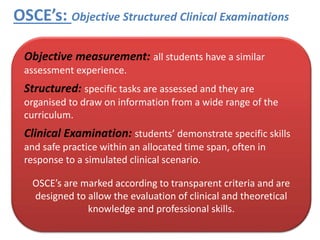
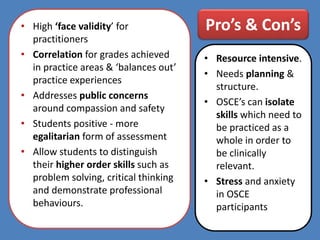
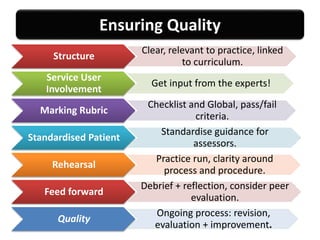
This document discusses the use of Objective Structured Clinical Examinations (OSCEs) in education. OSCEs aim to objectively assess students' demonstration of clinical skills and application of professional knowledge through a series of simulated scenarios. The document outlines the key components of OSCEs, including that they assess interpersonal skills, empathy, clinical reasoning and safe practice. Both the advantages and disadvantages of OSCEs are presented, such as their ability to evaluate a wide range of skills but also their resource intensiveness. Recommendations for ensuring quality in OSCE implementation include involving service users, using standardized patients, and providing students with practice and feedback opportunities.