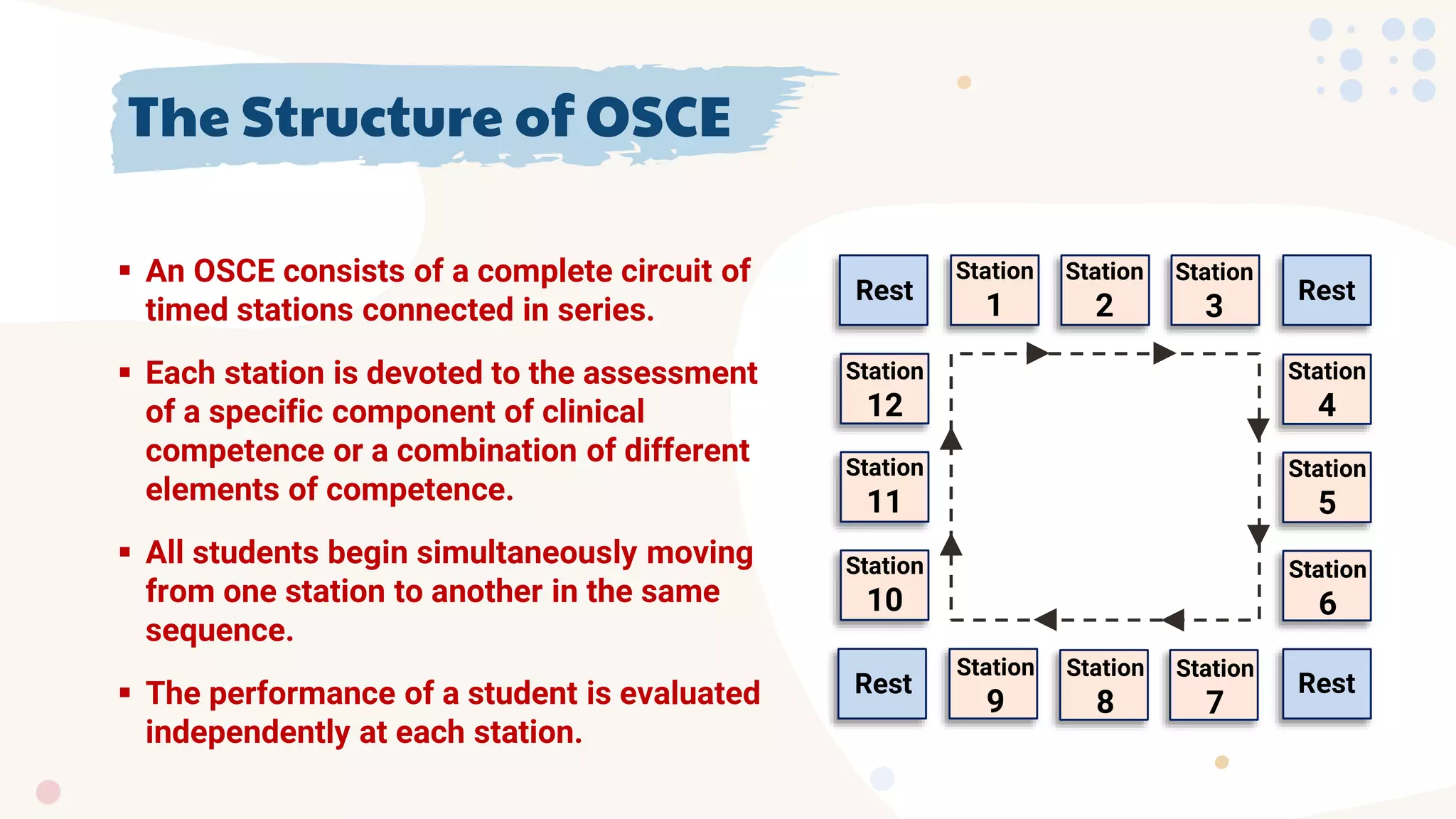
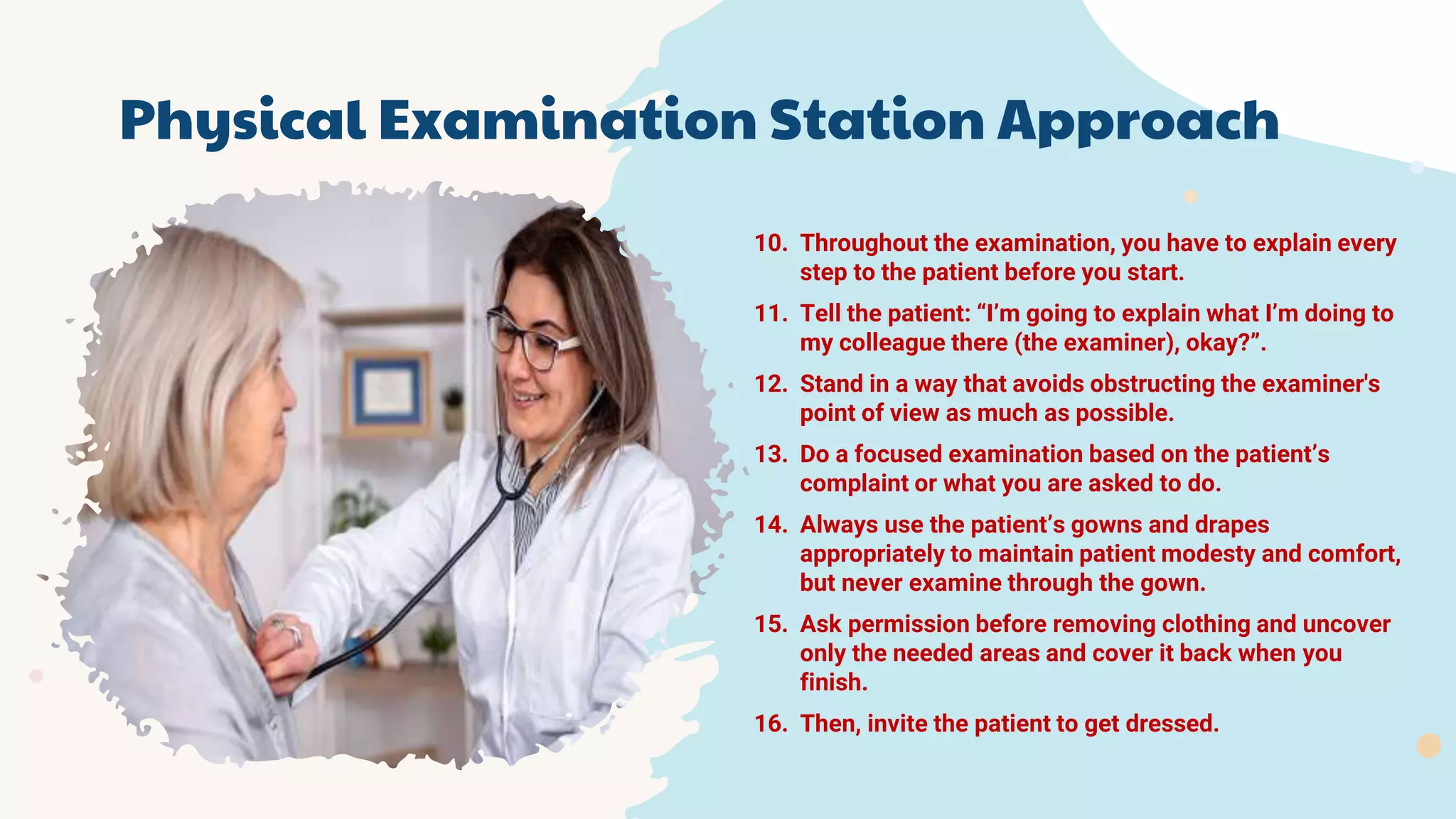
The document explains the Objective Structured Clinical Examination (OSCE), highlighting its role in assessing clinical competence through a series of timed stations that evaluate various skills like history-taking, physical examination, communication, and procedural skills. It provides a structured format to minimize subjectivity and aims for a standardized assessment of candidates' clinical performances. The document also details the specific approaches and strategies candidates should adopt to effectively navigate each OSCE station.