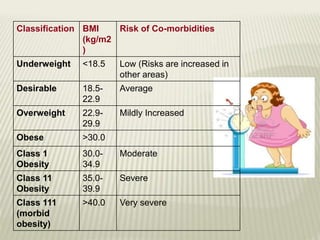
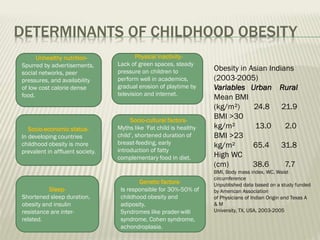
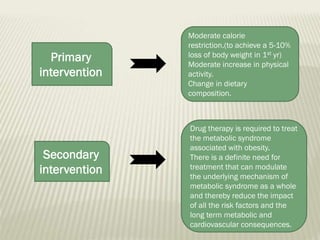
Obesity is defined as abnormal growth of adipose tissue due to enlargement of fat cells or increase in fat cell number. Central obesity is measured by waist circumference. Obesity is classified based on BMI and is associated with increased risk of comorbidities like diabetes, hypertension and dyslipidemia. It is caused by factors like unhealthy diet, physical inactivity, genetics and hormones. Treatment involves moderate calorie restriction and physical activity. Homoeopathic medicines like Calcarea carb, Natrum mur, Ammonium carb and Ferrum met can help in obesity management.






















































![Obesity by bijay [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesitybybijayautosaved-200407031519-thumbnail.jpg?width=640&height=640&fit=bounds)

































