Download as PDF, PPTX




















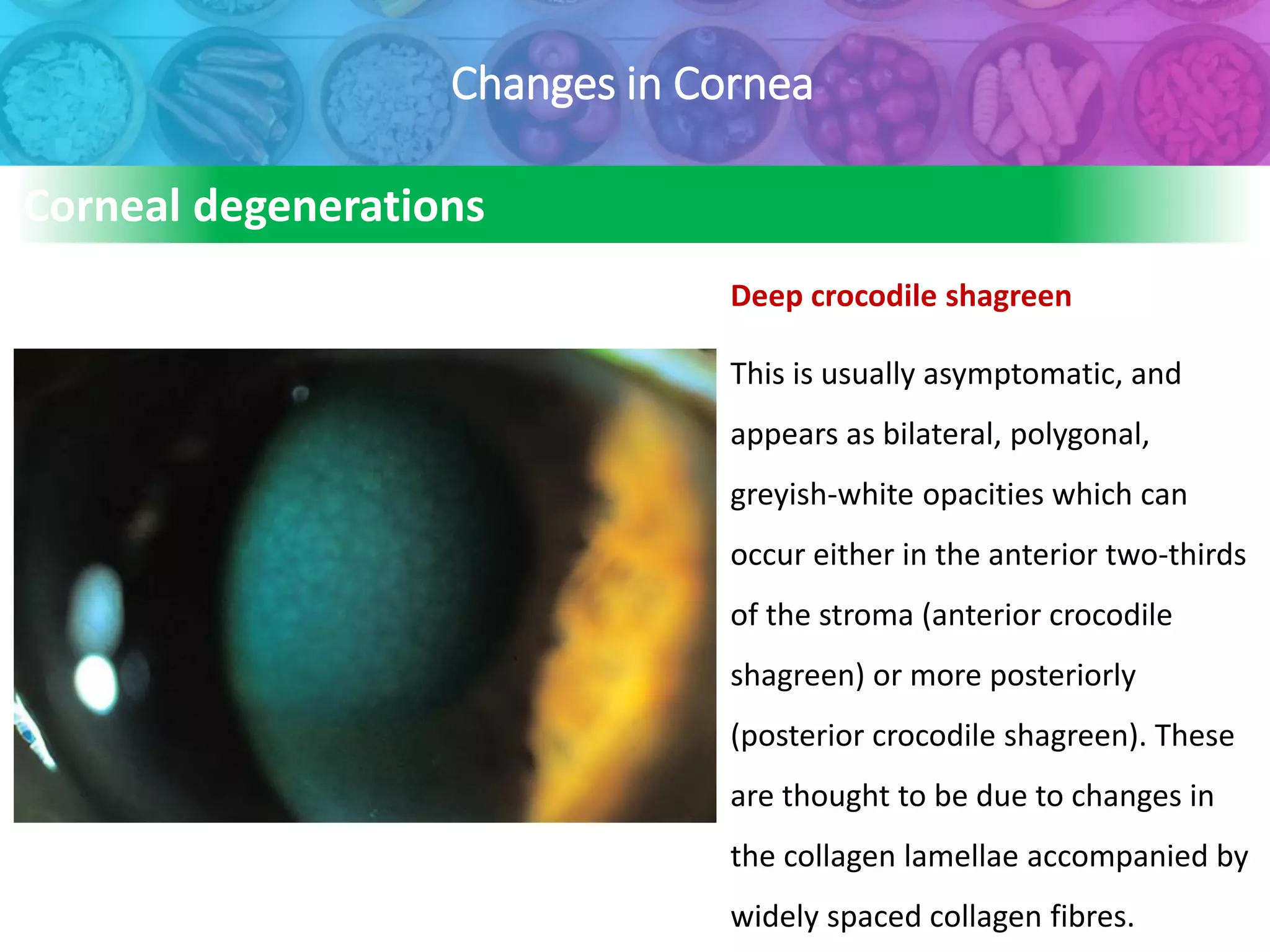




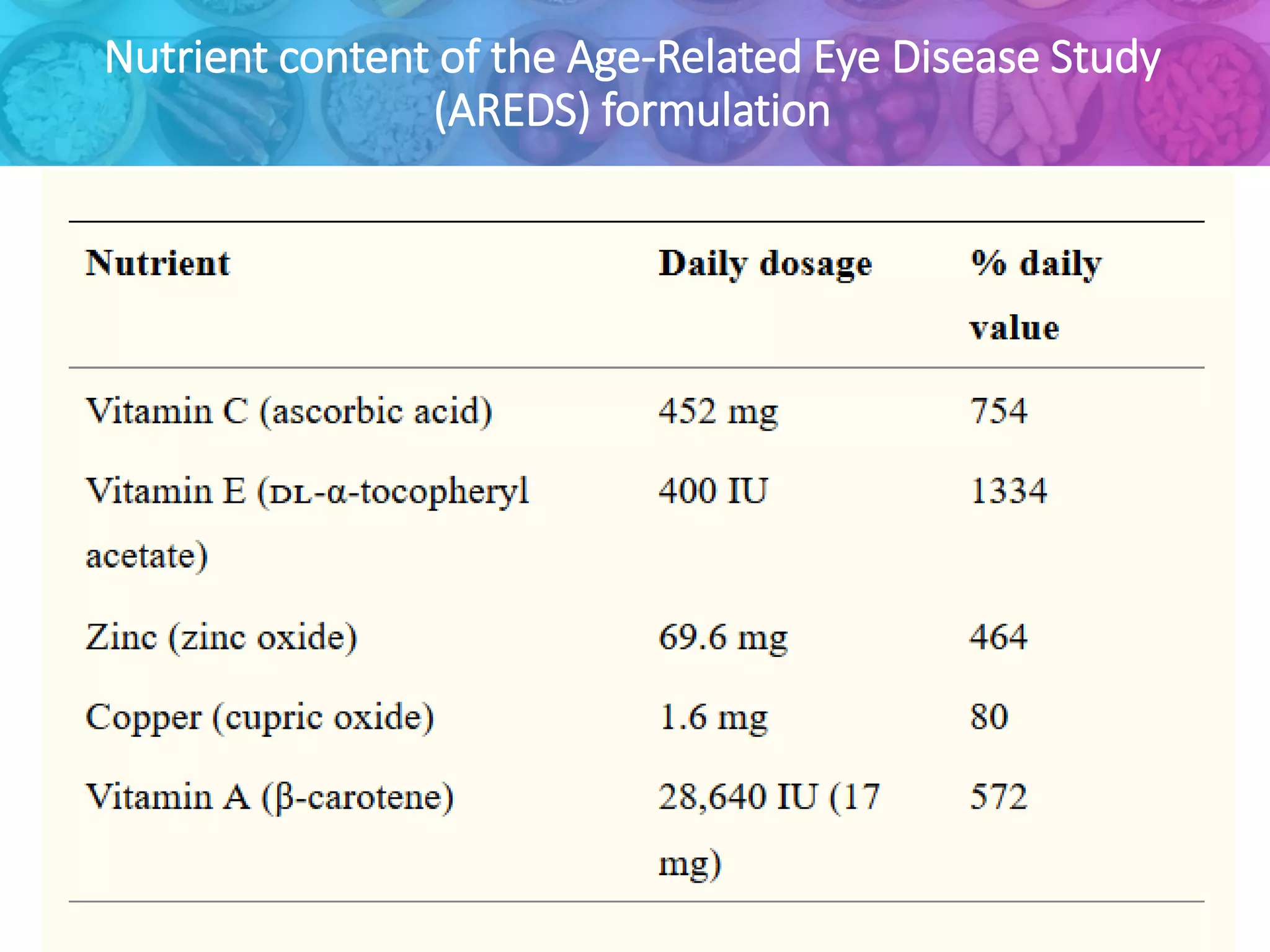
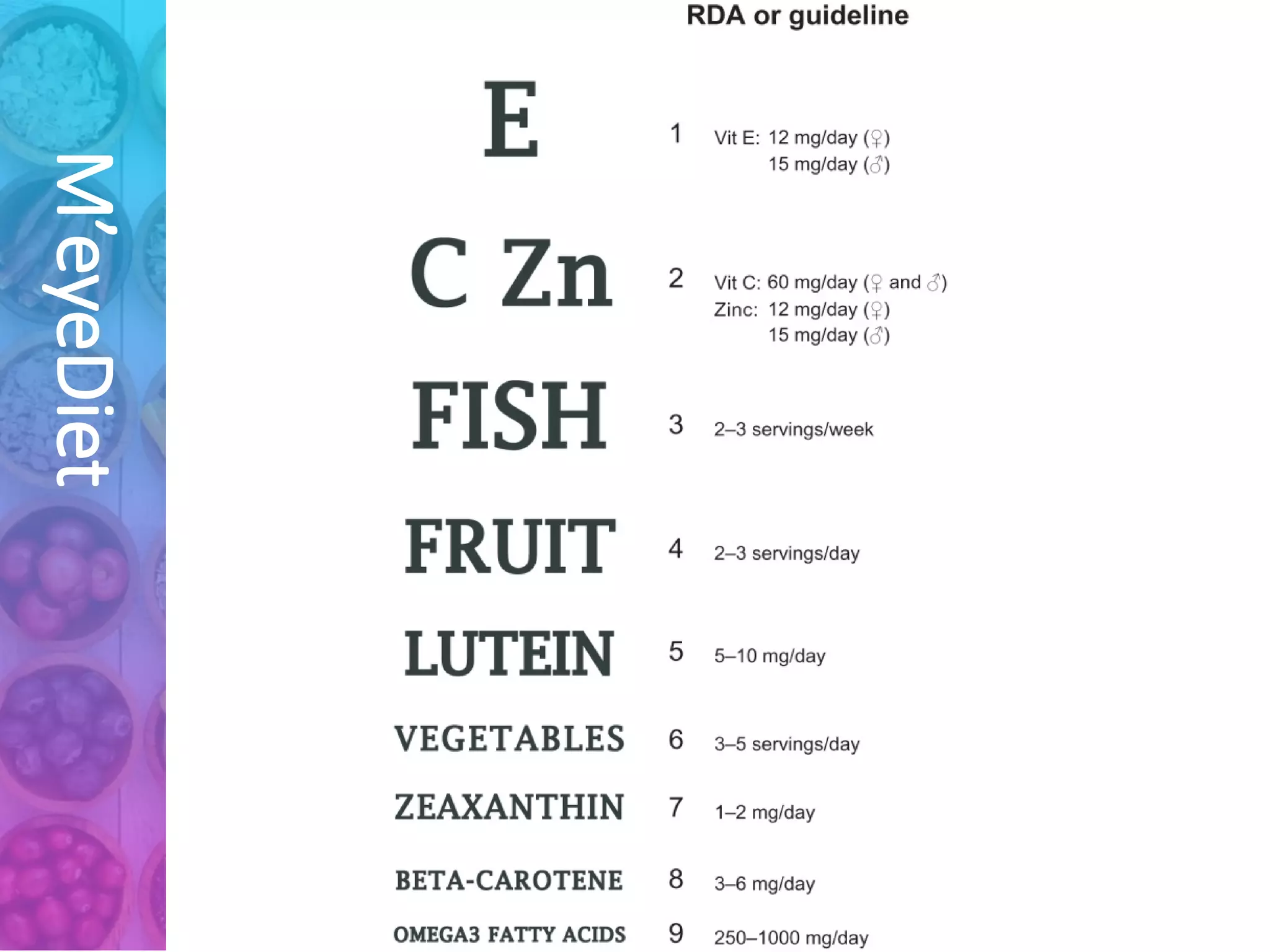

The document discusses the impact of aging on nutrition and ocular health, highlighting the relationship between aging processes and nutritional deficiencies in elderly individuals. It emphasizes that good nutrition, alongside physical activity, is crucial for maintaining health and independence among older adults, who are at heightened risk of malnutrition and various health issues due to factors like reduced appetite and changes in metabolism. Additionally, it reviews how aging affects ocular health, particularly in relation to changes in the cornea and vision, stressing the importance of addressing these nutritional needs to improve well-being in older populations.











































![Aging and bone health [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/agingandbonehealthautosaved-180918161728-thumbnail.jpg?width=640&height=640&fit=bounds)