
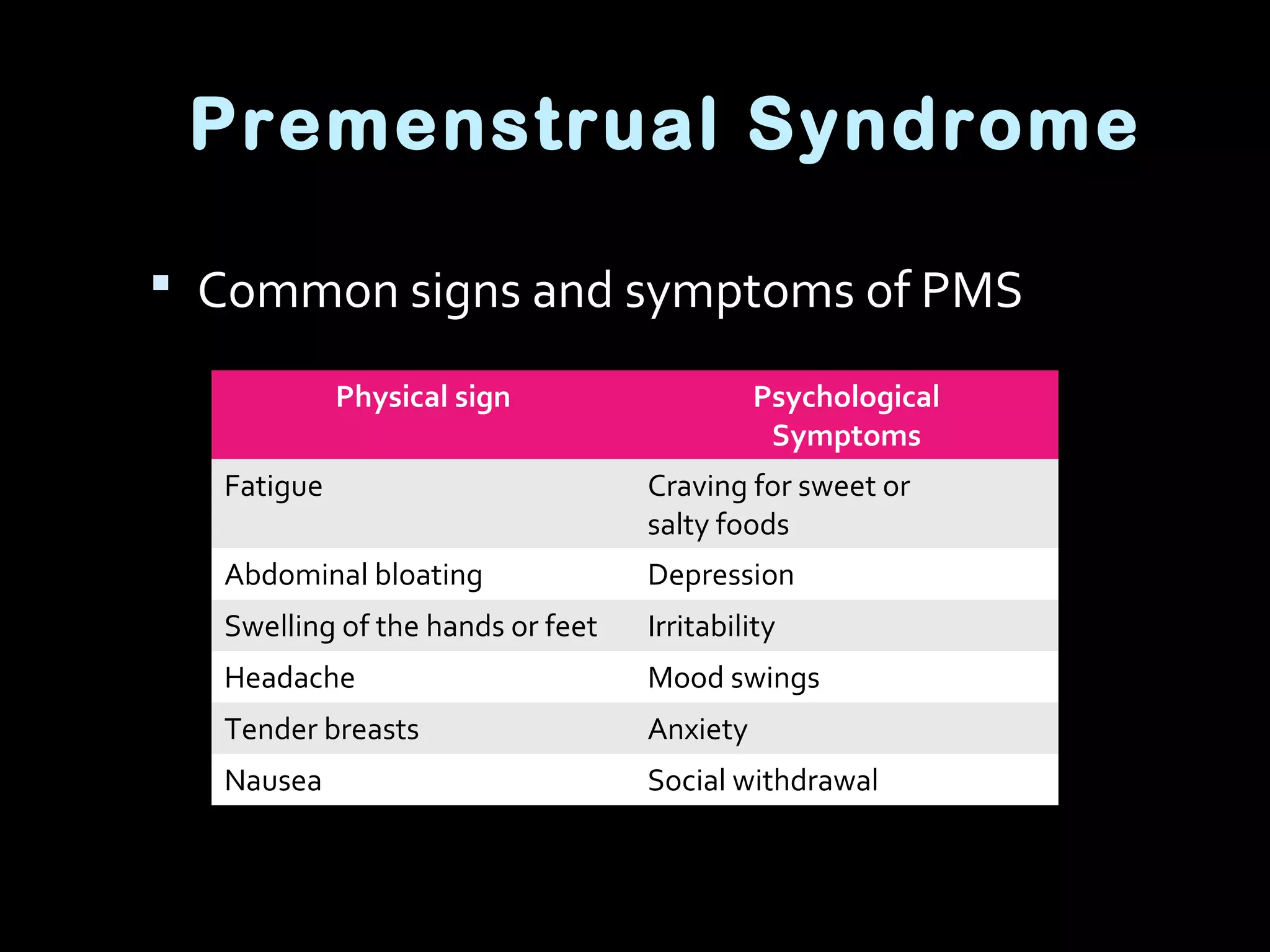


This document provides an outline for a course on preconception nutrition. It discusses topics like reproductive physiology, factors affecting fertility like nutritional status and contraceptive use, recommended nutrient intakes before conception, and conditions like PMS and obesity that can impact fertility. The key messages are that nutrition prior to conception is important for developing eggs and sperm and reducing risks during early pregnancy development. Maintaining a healthy weight and diet with adequate folate, iron and other nutrients can help support fertility and pregnancy outcomes.





































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





