Downloaded 895 times
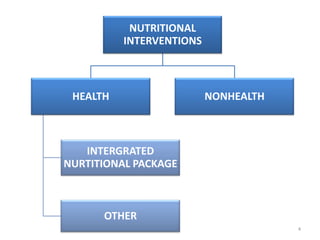
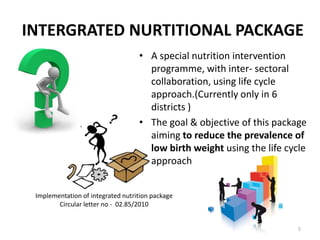
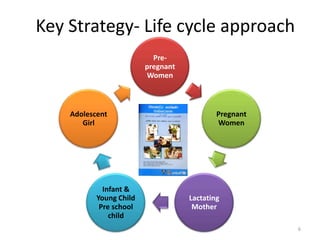
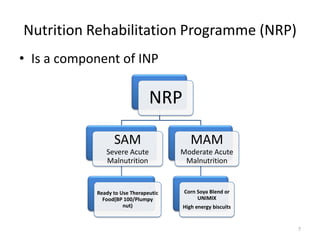



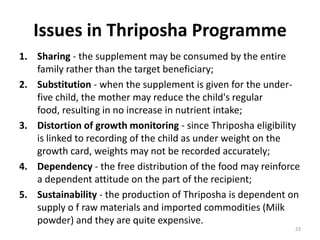

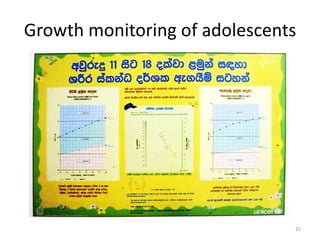

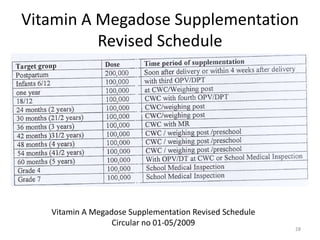

The document outlines various nutritional interventions aimed at improving health outcomes through planned actions targeting individuals, communities, and groups. It details components such as the integrated nutritional package, care protocols for pregnant and lactating mothers, and strategies for child nutrition and growth monitoring. Additionally, it discusses the challenges related to programs like Thriposha and Corn Soy Blend, including issues of compliance, targeting, and sustainability.





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

