Downloaded 29 times

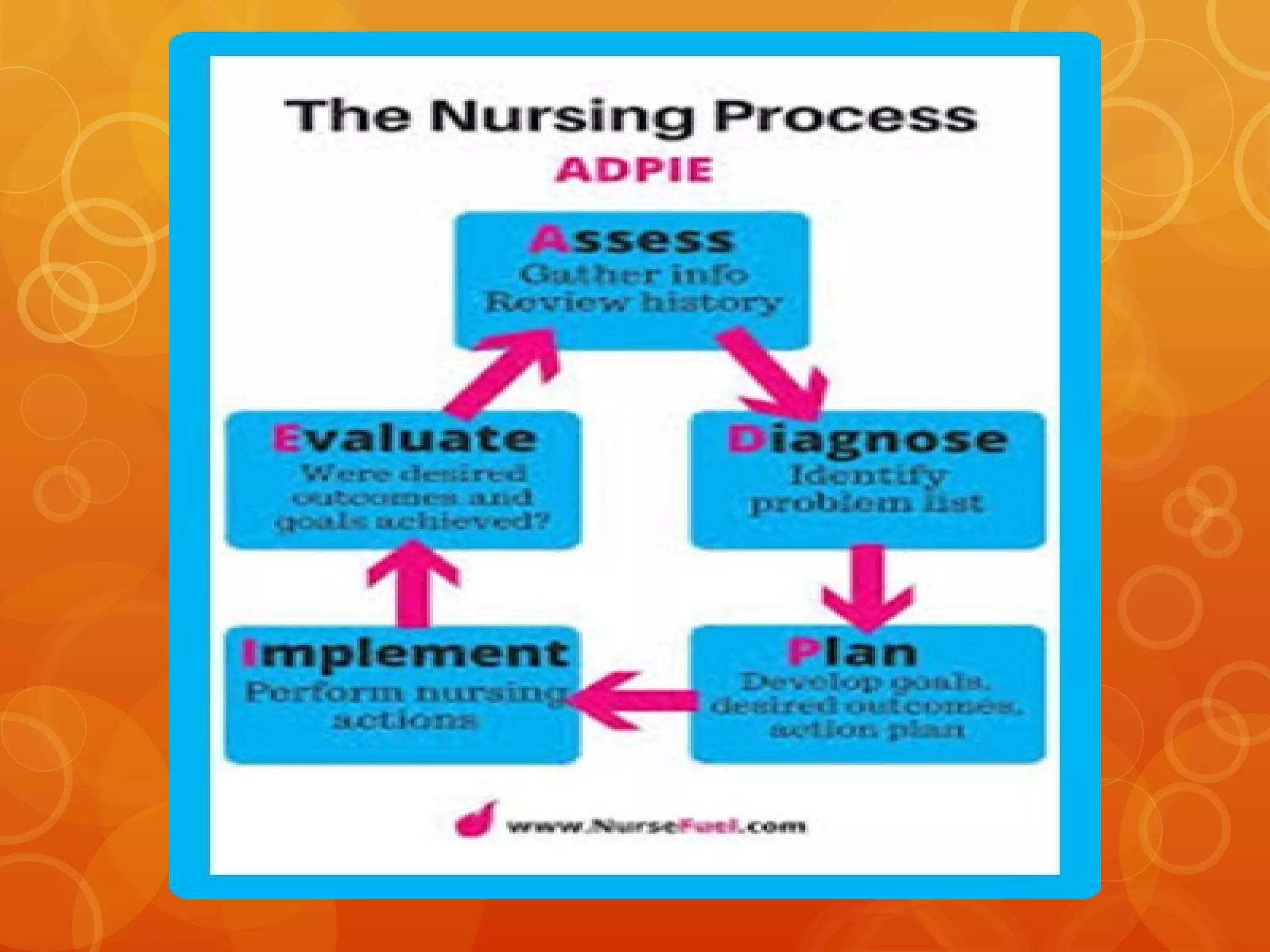
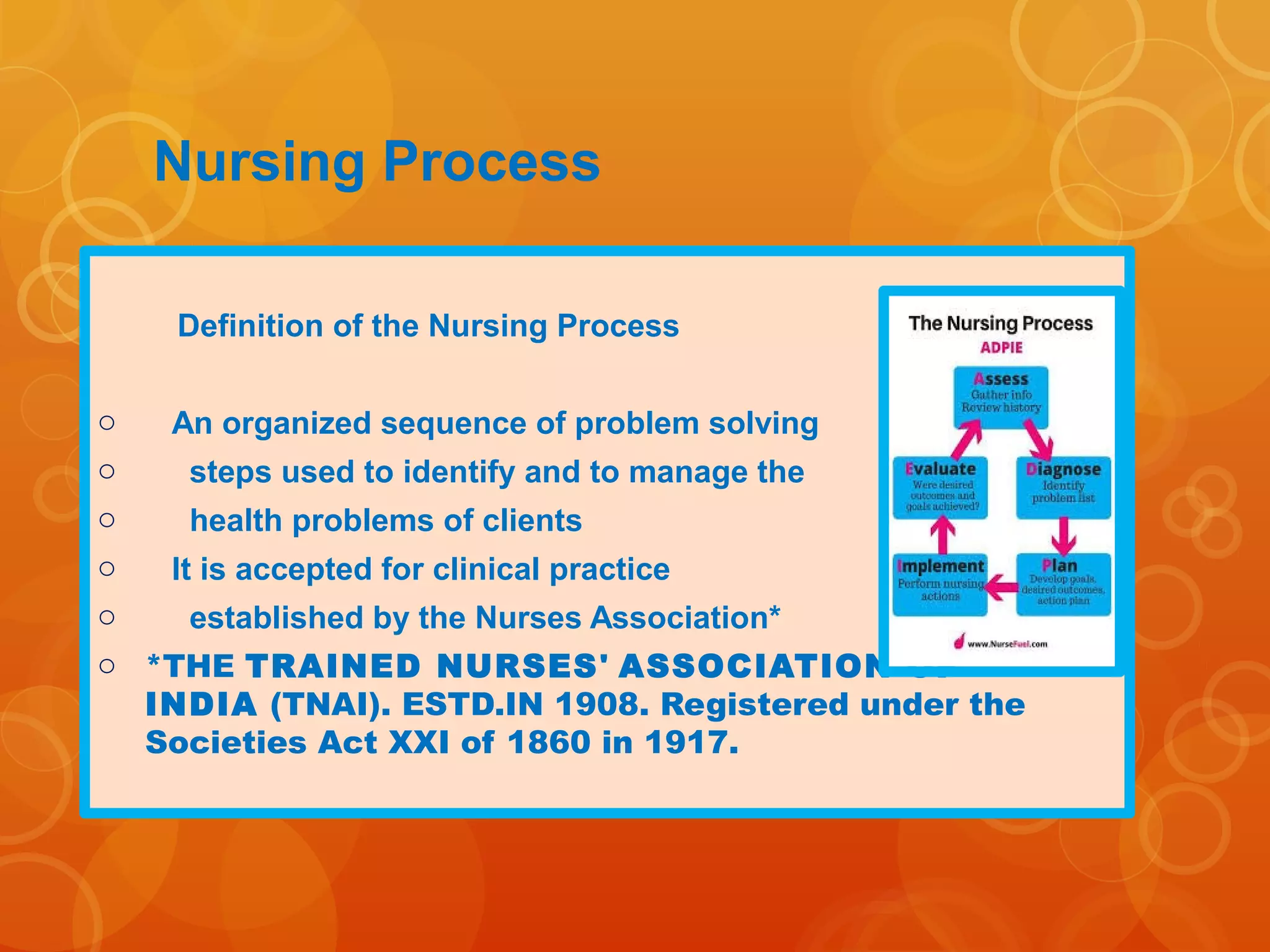
































































The nursing process is a framework that organizes nursing care through five steps: assessment, nursing diagnosis, planning, implementation, and evaluation. It provides an orderly and systematic method for planning and delivering nursing care centered around the client. The assessment step involves comprehensively gathering both subjective and objective data on the client's health, needs, and situation through various sources like interviews, examinations, and records.























































































