Introduction
• Practice ofnursing means caring which is directed
by the way the nurses view the client, the client's
environment, health and the purpose of nursing.
• Nursing process is a problem-solving approach
adapted by the nurse to assess the patient's needs
and provide evidence-based care.
• To nurses the nursing process provides a useful
description of how nursing should be performed.
3.
History of NursingProcess
• The term 'Nursing Process' was first mentioned by
'Lydia Hall, in 1955 with 3 STEPs process: Observation,
Administration of care and Validation.
• In 1967, Yura and Walsh further assessment to the
three steps and described a four-step process (APIE)
• In the mid-1970s an addition of diagnostic phase was
added resulted into a five-step process (ADPIE).
• American Nurses Association's Standards of Practice
included diagnosing as a function of professional
nursing in 1973.
• After 1980 the nursing process was added to the
General Nursing Curriculum in India.
4.
Meaning of NursingProcess
• The two words of nursing process are significant -
Nursing and Process.
• Nursing - providing care to the clients during illness
and assisting the client to achieve maximum health
potential.
• Process - a series of event which includes rational
thoughts, decisions and action to achieve a goal.
6.
Definition
• "The nursingprocess is systematic, goal directed,
Client-centered structured method for delivery of
nursing care."
• Professional nurses apply critical thinking process
to select the best available evidence to caregiving
and promoting human functions and responses to
health and illness.
• ~American Nurses Association, 2010.
7.
• Nursing Processis defined as systematic and
dynamic method of providing care to clients. It
comprises series of sequential phases built upon
the preceding step.
9.
Purpose of NursingProcess
• To provide a framework within which the nurse can
identify a client's health status and actual or
potential health care problems/needs
• To establish a plan of care to meet identified needs.
• To provide an individualized, holistic, effective and
efficient nursing
• To systematically evaluate the client response
based on the interventions provided.
• To help the nurse provide goal-directed, client-
centered care.
10.
Characteristics of NursingProcess
• Client Oriented: It is developed and implemented
taking into consideration the unique needs of the
individual client in providing care.
• Problem Oriented: Care plan are organized
according to client's problem. Problem can be
actual and potential.
• Goal Oriented: Goals and plan of care should be
based according to client's problems/needs
• Outcome Oriented: It is determined by the
expected outcome of a client's problem on the
basis of intervention provided.
11.
• Organized andSystematic: The nursing process is a
systematic method that directs the nurse to
determine the need for nursing care, in a
systematic and organized manner.
• Flexible: A nurse can adapt the nursing process in
any setting and area.
• Dynamic and Cyclic: Nursing process is a continuous
assessment and evaluation of client's response to
the applied nursing action
ASSESSMENT
• Assessment isthe first step in delivering nursing
care.
• Assessment is a systematic, dynamic process by
which the nurse collect and analyzes data.
14.
Purpose of Assessment
•To identify the actual and potential health problem
or needs of the client
• To organize a database according to the physical,
psychological and emotional health
• To formulate Nursing Diagnosis
• To ascertain the client's functional behavior
• To promote holistic nursing care
• To form a therapeutic interpersonal relationship
with the client
15.
Types of NursingAssessment
• Initial or Comprehensive
• Problem-Focused
• Emergency
• Time-Lapsed
16.
• INITIAL orCOMPREHENSIVE ASSESSMENT
• Initial/Comprehensive Assessment is performed within a
specified time duration after the admission. It is also
known as admission assessment.
• Purposes
• To obtain in depth comprehensive baseline data
regarding the client health status for evaluating changes
in the client's health status;
History Collection
Assessment of risk factors and coping strategies
Example: Risk for Fall, Pressure ulcer, Pain.
Head to toe examination including Vital Sign Monitoring
System wise assessment
17.
• PROBLEM-FOCUSED ASSESSMENT
•It is usually performed after the initial Assessment and
nurse gathers the data regarding the specific problem
that has already been identified.
• Purposes
• To get detail data related to the specific health problem
for which the patient admitted to the hospital.
• Patient is admitted with the chief complains of
polyuria, so focused assessment include renal system
specific assessment.
18.
• EMERGENCY ASSESSMENT
•It is a rapid assessment to be performed during any
physical or psychological crisis (Impairment of airway,
breathing and circulation).
• Purposes
• To identify the life-threatening problem
• In case of trauma :Primary & Secondary assessment
(Survey)
19.
• PRIMARY ASSESSMENT
•The acronym ABCDE
provides the basis of the
primary assessment.
• A: Airway
• B: Breathing
• C: Circulation
• D: Disability
• E: Exposure
• SECONDARY ASSESSMENT
• The main focus is to explore
specific medical conditions
• F: Full set of Vital sign
• G: Give comfortable position
• H: History taking and head to
toe assessment
• I : Inspection of the posterior
side of the body
20.
• Time-Lapsed Assessment
•Periodic time-lapsed assessments are done to reassess
health status and it is also known as ongoing assessment
• Purposes
• Compare a patient's current status to baseline data
obtained earlier in order to make necessary revisions in
the plan of care.
• Periodic Outpatient Clinic Visits.
• The ongoing assessment of the clinical parameter of
patient after admission.
Types of Data
•Subjective data: It is obtained directly from the
patient and elicits information about:
• How patient feels
• Difficulties of the patient
• Problems expressed by the patient
• Complaints of patient
• Objective data: Refers to information based on
observation of the nurse and examination of the
patient.
24.
Sources of Data
•Primary Source
• The data is gathered directly from the main source
of information.
• Patient is the primary source of information.
• Secondary Source
• It is used when the patient is not able to give the
information related to his/her own health condition
(Unconscious patient or trauma patient with airway
compromised)
• Secondary source includes patient family member,
friends, Diagnostic and lab reports.
25.
Method of Datacollection
• History Collection
• Physical Examination
• Diagnostic or lab test report
26.
Method of DataCollection-
History Collection
• A semi-structured interview process to collect a detailed
health record of the patient.
• Component of History Collection
• Chief Complaint
• Present Medical History
• Past Medical History & Surgical History
• Family History
• Obstetrical History (In case of female patient)
• Personal History
• Occupational History
• Drug and Allergic History
27.
Method of DataCollection-
Physical Examination
• The physical examination is a systematic data collection
method to detect the patient health problems.
• Inspection
• E.g.: Cyanosis
• Palpation
• E.g.: Lymph nodes
• Percussion
• E.g. Presence or absence of fluid
• Auscultation
• E.g.: Abnorma breath
28.
2.Organization of Data
•The data collected from the patient is then
organized systematically either by using a written or
computerized format.
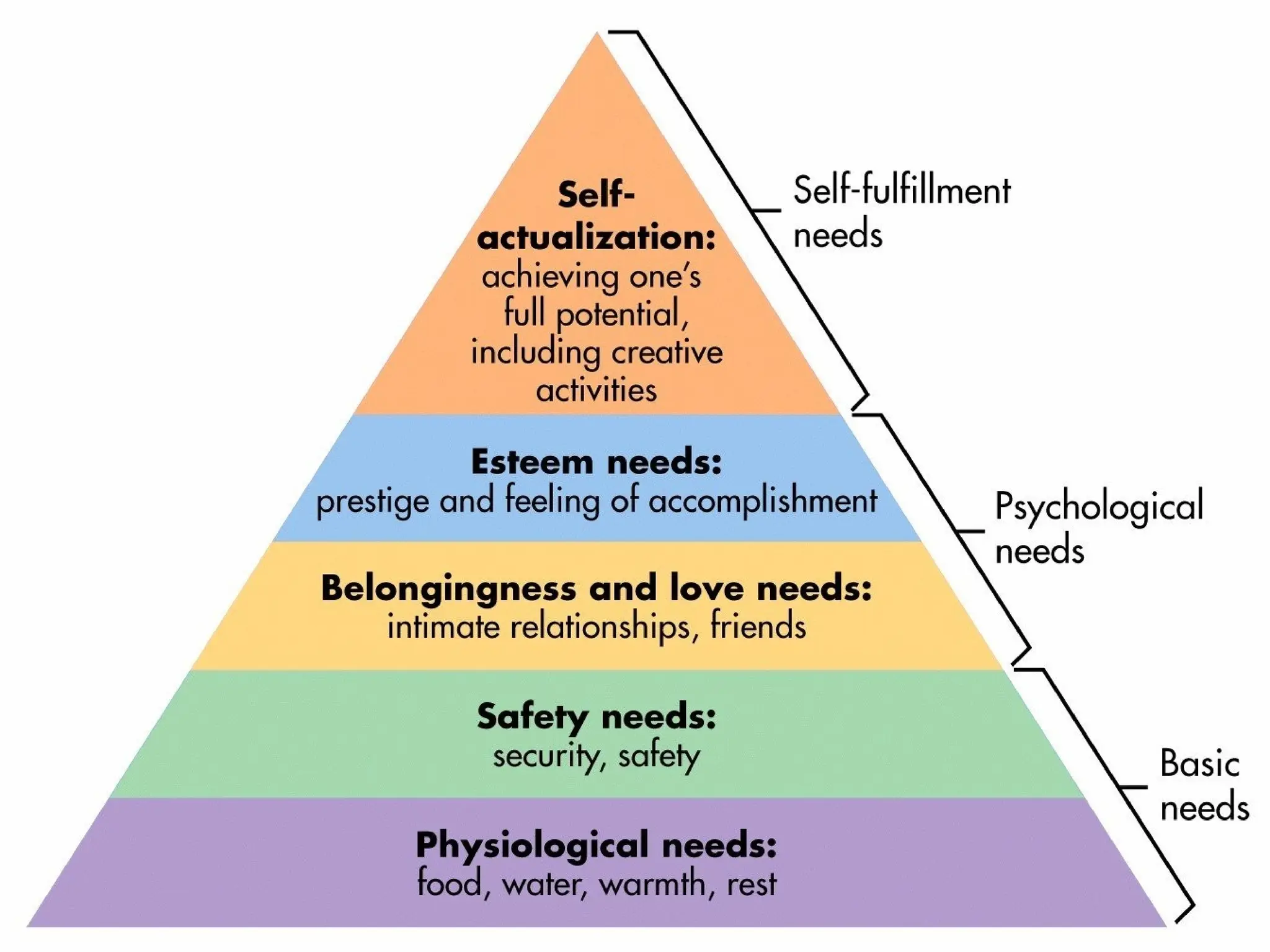
• The data is organized on the basis of the following:
• Maslow Hierarchy of need
30.
• Body systemsmodels: Organized the data according to
the tissues and organ function in the various body
systems.
• Gordon's Functional health pattern provides a
framework for data collection mainly focusing on 11
functional health pattern.
• Health Perception, Nutritional Pattern, Elimination
Pattern, Activity Pattern, Cognition Pattern, Sleep
Pattern, Self Concept Pattern, Relationship Pattern,
Reproductive Pattern, Copping Pattern, Value Beliefs
Pattern.
• Theory of Self-care: Dorothea Orem's theory of self
care focuses on identifying the client ability to meet
the self-care needs & identifying self-care deficit.
31.
3.Validate the data
•Data collected during the assessment needs to be
validated in order to check the accuracy and quality
of source data before using the obtained data.
• Purposes
• To ensure the data collection is complete
• To make sure that the subjective and objective data
collected should reliable and accurate.
32.
4.Documentation of Data
•Accurate documentation is an integral part of all the phases of
nursing process to enhance effective, accurate and individualized
patient care.
• Purposes
• ➤ To communicate the information to other health care providers
• ➤ To provide a legal record
• ➤ To act as a safeguard for the health care providers
• To provide framework for formulating the nursing diagnosis
• ➤ To avoid misunderstanding
• ➤ Offer research topics for future studies
33.
Nursing Diagnosis
• "Nursingdiagnosis is a clinical judgment about
individual, family, or community responses to
actual or potential health problems/life processes.
Nursing diagnosis provides the basis for selection of
nursing interventions to achieve outcomes for
which the nurse is accountable."
• ~Official NANDA definition 1990
34.
• NURSING DIAGNOSISIN A NUTSHELL
• Nursing Diagnosis: "Frame of reference from
which nurses could determine what to do
and what to expect" in a clinical situation.
35.
History of NursingDiagnosis
• In 1953, Virginia Fry and R Louise McManus introduced the
term "nursing diagnosis" to describe a step necessary in
developing a nursing care plan.
• In 1972, the New York State Nurse Practice Act identified
diagnosing as part of the legal domain of professional
nursing.
• In 1973, the development of nursing diagnosis formally
began when two faculty members of the Saint Louis
University, Kristine Gebbie and Mary Ann Lavin, perceived a
need to identify nurses' roles in ambulatory care settings.
• Also in 1973, the American Nurses Association's Standards
and included diagnosing as a function of professional
nursing.
36.
• In 1980,ANA Social Policy Statement defined nursing as:
"the diagnosis and treatment of human response to
actual or potential health problems."
• International recognition of the conferences and the
development of nursing diagnosis came with the First
Canadian Conference in Toronto (1977) and the
International Nursing Conference (1987) in Alberta,
Canada.
• In 1982, the conference group accepted the name "North
American Nursing Diagnosis Association (NANDA)". In the
same year, the newly-formed NANDA used "nine patterns
of unitary man" as an organizing principle.
• In 1984, NANDA renamed "patterns of unitary man" as
"human response patterns" based on the work of
Marjorie Gordon.
37.
• In 1997,NANDA changed the name of its official journal
from "Nursing Diagnosis" to "Nursing Diagnosis: The
International Journal of Nursing Terminologies and
Classifications."
• In 2002, NANDA changed its name to NANDA
International (NANDA-I) to further reflect the
worldwide interest in nursing diagnosis. In the same
year, Taxonomy I was revised & Taxonomy II version of
Gordon's Functional health patterns introduced.
• As of 2018, NANDA-I has approved 244 diagnoses for
clinical use, testing, and refinement.
38.
Characteristics of Nursing
Diagnosis
•Reflects a clear and concise health problem
• Provides a basis for planning and other steps of
nursing process
• Provides a complete overview of patient's problem
• Defines nursing's unique boundaries with respect
to medical diagnoses
39.
Purposes of NursingDiagnosis
• It helps in identifying nursing priorities and helps in
providing nursing interventions based on identified
priorities.
• It helps in the formulation of expected outcomes for
quality assurance.
• Provides a basis of evaluation to determine if nursing
care was beneficial to the client and cost-effective.
• Nursing diagnoses are an effective teaching tool to
help nursing students to sharpen their problem-
solving and critical thinking skills.
40.
Difference between Nursingand
Medical diagnosis
NURSING DIAGNOSIS
It is based on comprehensive and
holistic needs of the patient
The goal of nursing diagnosis is to
identify the actual and potential
health problem
It describes the problem treated by
the nurse by providing dependent
and independent nursing action
It changes as per the patient response
toward the intervention applied by
the nurse.
It is formulated based on the actual,
possible, associated risk factors of
nursing diagnosis
Examples: Ineffective Breathing
MEDICAL DIAGNOSIS
It is based on the physical,
biological and psychological aspects
of the patient
The goal of medical diagnosis is to
find out the exact cause of illness or
injury and design a treatment plan
It is considered as the problem of
which the physician directs the
primary treatment.
It remains constant until the cure is
effec
It is based on the sign and
symptom of the patient.
Example: Asthma
41.
Types of nursingdiagnosis
1). Problem focused nursing diagnosis
2). Risk nursing diagnosis
3). Health promotion nursing diagnosis
4). Syndrome nursing diagnosis
42.
Problem-Focused Nursing
Diagnosis
• Aproblem-focused diagnosis is also known as
actual diagnosis.
• It is based on the patient's problem & sign and
symptoms which is present at the time of the
nursing assessment.
• Actual nursing diagnoses should not be viewed as
more important than risk diagnoses. There are
many instances where a risk diagnosis is considered
the highest priority for a patient.
43.
• Problem-focused nursingdiagnoses have three components:
• Diagnosis label or problem
• Related factors
• Defining characteristic
• Examples of actual nursing diagnosis are:
• Ineffective breathing pattern related to ventilation perfusir
mismatch as evidenced by change in respiratory rate and
dyspnea, Cyanosis, decreased PO2 and SaO2; increased
PCO₂
44.
Risk Nursing Diagnosis
•Risk Nursing Diagnoses are the clinical judgment to
be made by the nurse regarding a problem that
does not exist, but the presence of risk factors
indicates that a problem is likely to develop unless
nurses intervene.
• For example, an unconscious patient who is
confined to bed is in the risk of developing the
pressure ulcer.
45.
Health Promotion Diagnosis
•Health promotion diagnosis is also known as
wellness diagnosis.
• It is a clinical judgment related to motivation and
desire to enhance the patient well-being.
• Health promotion diagnosis is concerned with the
individual, family, or community transition from a
specific level of wellness to a higher
• level of wellness.
46.
• Components ofa health promotion diagnosis
generally include only the diagnostic label or a one-
part-statement.
• Examples of health promotion diagnosis:
• Readiness for Enhanced Spiritual Well Being
• Readiness for enhanced self esteem
• Readiness for Enhanced Family Coping
47.
Syndrome Diagnosis
• Asyndrome diagnosis is a clinical judgment
describing a specific
• cluster of problem
• Components of a health promotion diagnosis
generally include only the diagnostic label or a one-
part-statement.
• Chronic Pain Syndrome
• Post-trauma Syndrome
48.
Possible Nursing Diagnosis
•• A possible nursing ng diagnosis is not a type type
of diagnosis but it describe a suspected problem for
which additional data required to confirm or rule
out the suspected problem.
• Examples include
• ➤Possible Chronic Low Self-Esteem
• ➤Possible Social Isolation.
• Impaired PhysicalMobility
• Impaired Skin Integrity
• Impaired Urinary Elimination
• Impaired Verbal Communication
• Ineffective Airway Clearance
• Ineffective Breathing Pattern
• Ineffective Coping (Maladaptive Coping)
• Ineffective Health Maintenance (Ineffective Health Self-Management)
• Ineffective Tissue Perfusion (Ineffective Peripheral Tissue Perfusion)
• Insomnia (Ineffective Sleep Pattern)
• Knowledge Deficit (Inadequate Health Knowledge)
• Risk For Aspiration
• Risk for Bleeding (Risk For Excessive Bleeding)
• Risk for Electrolyte Imbalance (Risk For Impaired Water-Electrolyte Balance)
• Risk for Falls (Risk For Adult/Child Falls)
• Risk for Infection
• Risk for Injury (Risk For Physical Injury)
• Risk For Unstable Blood Glucose (Risk For Ineffective Blood Glucose Pattern Self-Management)
• Self-Care Deficit (Decreased Self-Care Ability Syndrome)
• Social Isolation (Inadequate Social Connectedness)
• Urinary Retention (Risk For Urinary Retention)
51.
Planning
• Planning isa deliberate and systematic phase of
nursing process which involves decision making and
problem solving.
• It is the process of formulating patient goals by
using the assessment and diagnostic data and
designing the nursing interventions required to
prevent, reduce, or eliminate the patient's health
problems.
Principles of Planning
•Planning should be done on the basis of clearly
defined objectives
• It should be precise in its objective, scope and
nature
• Planning should follow hierarchical nature
• It should be flexible & continuous
• It should focus on expected outcomes.
54.
Advantages of Planning
•It provides a direction to specified nursing care
• It helps in faster achievement of goals in an
effective manner
• It provide a flow of control in an organization
• It eliminates the chances of uncertain decisions
• Cost effective
55.
Establishing Goals
• Apatient goal is desired outcome or change in
patient's behavior in the direction of health.
• Goal attainment reflects the resolution of the
patients concern or health problem that is specified
in the nursing diagnosis.
• The nursing diagnosis guides the type of goal
attainment: goals may reflect health restoration,
health maintenance or health promotion
56.
The purpose ofpatient goal is to:
• Provide direction for planning nursing interventions that will achieve the
anticipated changes in the patient.
• Provide direction for establishing evaluation criteria to measure the
effectiveness of the interventions.
• Examples of patient goals:
• The patient/client will
• Restore fluid volume.
• Increase actively tolerance.
• Maintain urinary elimination pattern.
• Decrease potential for injury.
• Develop coping abilities.
• Improve nutritional pattern.
• Increase parental knowledge.
• Establish change in family roles.
57.
Types of Planning
•1. Initial Planning
• 2. Ongoing Planning
• 3. Discharge Planning
• 1. Initial Planning : Planning which is done after the
initial assessment.
• 2. Ongoing Planning: It is a continuous planning.
• 3. Discharge Planning : Planning for needs after
discharge
58.
Steps in PlanningNursing Care
• 1. Determining priorities: This involves analyzing the
problems identified in the assessment stage, to decide
which problem requires priority of attention. This
involves judgments made in relation to the impact of
each nursing diagnosis for that client's/family's
immediate and long-term well-being.
• 2. Setting goals: These state what is to be achieved if the
identified problems are to be alleviated.
• 3. Selecting nursing actions: This involves choosing the
methods and techniques which will enable us to achieve
the stated patient's goal.
• 4. Writing the care plan: The problems, goals and
nursing actions are recorded on the nursing care plan.
59.
Implementation
• Implementation consistsof doing and
documenting the activities.
• Use cognitive, technical, interpersonal and
ethical skills to implement a plan of care
60.
•The process ofimplementation
includes;
•Implementing the nursing interventions
•Documenting nursing activities
61.
Categories of NursingActions
• Independent Nursing Actions:- These actions are initiated
by the nurse based on nursing knowledge and skills.
These actions are the result of the assessment of client
needs and may be initiated without the direction or
supervision of another health care professional.
• Dependent Nursing Actions:- These actions are carried
out according to specific routines, under the supervision
of a physician, or as a result of an order by a physician.
• Collaborative and Interdependent Nursing Action:- These
are performed either as a result of joint decision by a
nurse or another health team member.
62.
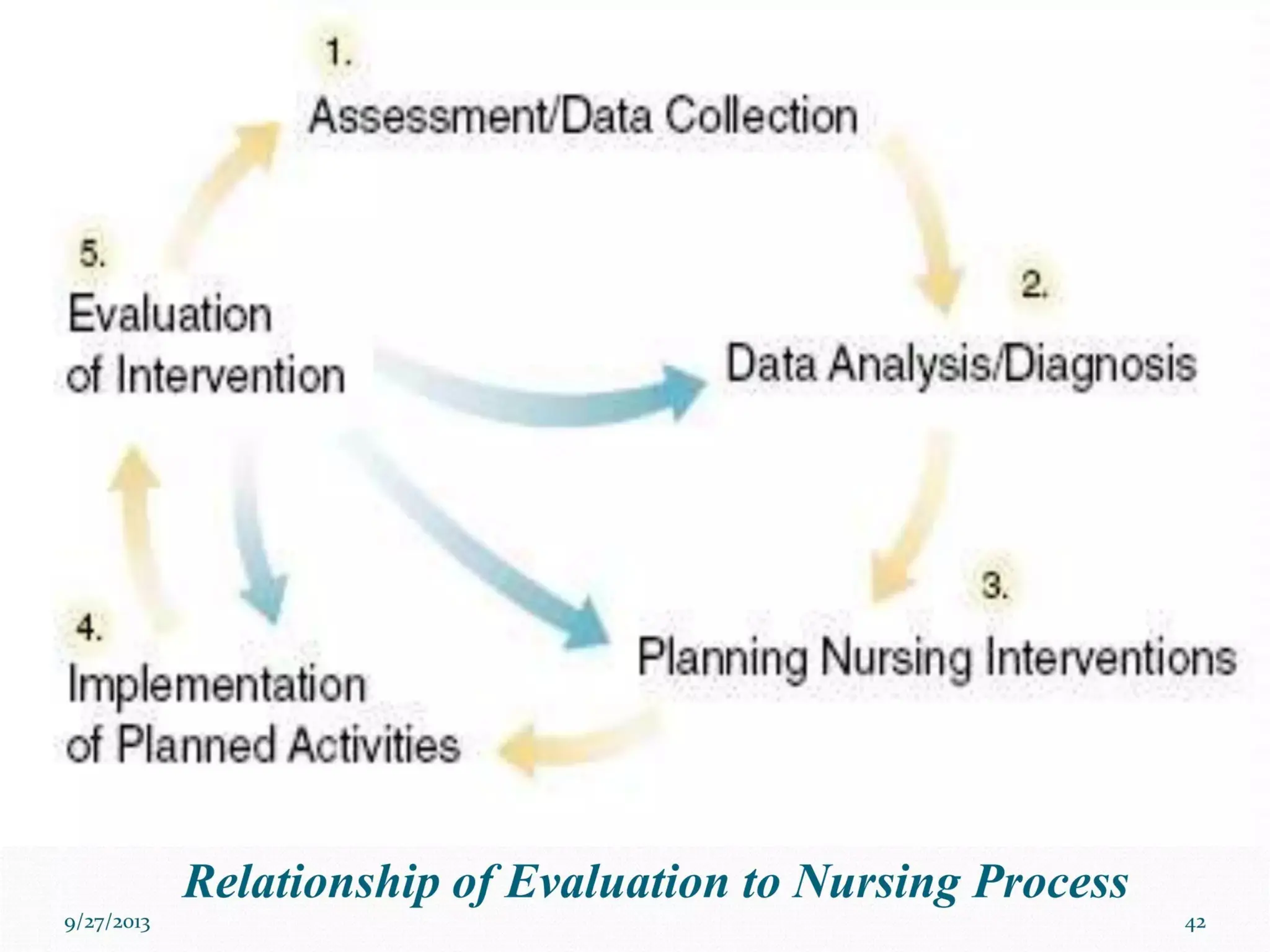
Evaluation
Evaluation is aplanned, ongoing, purposeful activity
in which the nurse determines;
(a)the client's progress toward achievement of
goals/outcomes and
(b)the effectiveness of the nursing care plan.
63.
• The evaluationincludes;
• Comparing the data with desired outcomes
• Continuing, modifying, or terminating the
nursing care plan.
64.
Purpose of Evaluation
•To compare patient response to applied nursing
intervention with the preset outcome criteria
• To assess the extent to which the patient goals
were achieved
• To identify the need to modify the nursing
intervention based on the patient response
• To assess the effectiveness of nursing care plan
• To assess for errors and quality of nursing care.