Downloaded 27 times




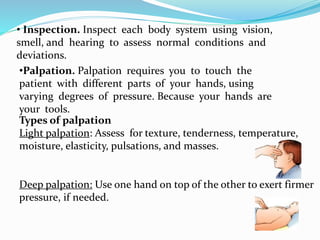
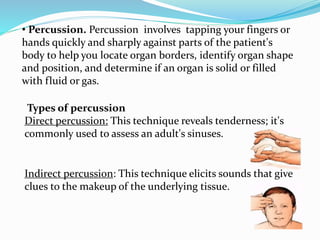









This document discusses the process of nursing assessment which includes physiological, psychological, social, and lifestyle factors. It describes the techniques used in physical assessment: inspection, palpation, percussion, and auscultation. It also discusses establishing nursing diagnoses, developing a care plan with goals, implementing care, documenting care, and evaluating the effectiveness of the care plan.