Nsh management of acne guidelines jan 2015
•
5 likes•3,995 views

NSH management of acne guidelines jan 2015 http://www.lambethccg.nhs.uk/news-and-publications/meeting-papers/lambeth-borough-prescribing-committee/Lambeth%20Borough%20Prescribing%20Committee/Clinical%20Guidelines/Management%20of%20Acne%20Guidelines%20Jan%202015.pdf

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Nsh management of acne guidelines jan 2015
Similar to Nsh management of acne guidelines jan 2015 (20)
More from Utai Sukviwatsirikul
More from Utai Sukviwatsirikul (20)
Recently uploaded
Recently uploaded (20)
Nsh management of acne guidelines jan 2015
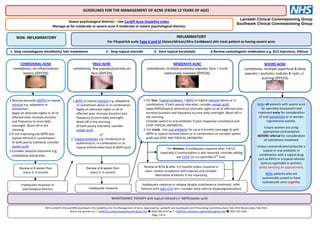
- 1. Lambeth Clinical Commissioning Group Southwark Clinical Commissioning Group GUIDELINES FOR THE MANAGEMENT OF ACNE (FROM 12 YEARS OF AGE) NON- INFLAMMATORY INFLAMMATORY For Fitzpatrick scale Type V and VI (Asian/African/Afro-Caribbean) skin treat patient as having severe acne COMEDONAL ACNE comedones, no inflammatory lesions (©PCDS) MILD ACNE comedones, few papules/pustules on face (©PCDS) MODERATE ACNE comedones, multiple pustules/ papules, face + trunk extensively involved (©PCDS) SEVERE ACNE comedones, multiple superficial & deep papules + pustules, nodules & cysts +/- scarring (©PCDS) 1.Benzoyl peroxide (BZPO) or topical retinoid e.g. adapalene or isotretinoin. Apply on alternate nights to all of affected area. Increase duration and frequency to once daily overnight. Wash off in the morning. 2.If not improving use BZPO and topical retinoid in combination. (If both poorly tolerated, consider azelaic acid). 3.Consider physical treatment e.g. comedone extraction. Review at 8 weeks then every 3- 4 months 1.BZPO or topical retinoid e.g. adapalene or isotretinoin alone or in combination. Apply on alternate nights to all of affected area. Increase duration and frequency to once daily overnight. Wash off in the morning. (If both poorly tolerated, consider azelaic acid) +/- 2. Topical antibiotic e.g. clindamycin or erythromycin; in combination or as topical antimicrobial (am) & BZPO (pm) Review at 8 weeks then every 3- 4 months Inadequate response or psychological distress Inadequate response 1.For face: Topical antibiotic + BZPO or topical retinoid (alone or in combination; if both poorly tolerated, consider azelaic acid). Apply BZPO/topical retinoid on alternate nights to all of affected area. Increase duration and frequency to once daily overnight. Wash off in the morning. Consider switch to oral antibiotic if poor response/ compliance and STOP TOPICAL ANTIBIOTIC. 2. For trunk: Use oral antibiotic for up to 6 months (see page 4) with BZPO or topical retinoid (alone or in combination or consider azelaic acid) and STOP ANY TOPICAL ANTIBIOTIC. Review at 8/52 & after 3-4 months unless response is poor; review compliance with topicals and consider alternative antibiotic if not improving Inadequate response or relapse despite maintenance treatment: refer. Patients with type V/VI skin: consider early referral (hyperpigmentation). Assess psychological distress – Use Cardiff Acne Disability Index. Manage as for moderate or severe acne if moderate or severe psychological distress. MAINTENANCE THERAPY with topical retinoid (+/- BZPO/azelaic acid) NHS Lambeth CCG and NHS Southwark CCG Guidelines for the Management of Acne. Approved by: Lambeth and Southwark Joint Prescribing Committee Date: Feb 2014 Review date: Feb 2016 Direct any queries to: LAMCCG.medicinesoptimisation@nhs.net 0203 049 4197 or SOUCCG.medicines-optimisation@nhs.net 0207 525 3253 Page 1 of 4 1. Stop comedogenic emollients/ hair treatments 2. Stop topical steroids 3. Start topical keratolytic 4.Review comedogenic medication e.g. B12 injections, lithium Refer all patients with severe acne for specialist assessment and treatment early for consideration of oral isotretinoin or in women cyproterone acetate. Ensure women are using appropriate contraception BEFORE referral for consideration of isotretinoin treatment Unless contraindicated prescribe a topical or oral antibiotic in combination with a topical drug such as BZPO or a topical retinoid (and co-cyprindiol in women) whilst awaiting an appointment. Refer patients who are systemically unwell or have nodulocystic acne urgently. For Women, if inadequate response after 3-4/12, especially if contraception is also required, consider adding any COCP (or co-cyprindiol 2 nd line) .
- 2. References: 1. © Cardiff Acne Disability Index. R J Motley, A Y Finlay 1992 (http://www.dermatology.org.uk/quality/cadi/quality-cadi.html); 2. NICE Clinical Knowledge Summaries (CKS) - Acne vulgaris (http://cks.nice.org.uk/acne-vulgaris#azTab) Last accessed May 2013; 3 British National Formulary 65 March-September 2013 Online (http://www.bnf.org/bnf/index.htm); 4. NICE Academic Detailing Aid: Minocycline use in acne; May 2012 (http://www.nice.org.uk/media/7EE/50/AcademicDetailingAidMinocyclineUseInAcne.pdf); 5. NHS England and Wales Drug Tariff May 2013 (http://www.ppa.org.uk/edt/May_2013/mindex.htm); 6. Primary Care Dermatology Society Guidelines (http://www.pcds.org.uk/clinical-guidance/acne-vulgaris) (SEE FOR IMAGES) Acknowledgements: This document was developed by clinicians of NHS Lambeth CCG, NHS Southwark CCG and; Departments of Dermatology at GSTT and KCH:Dr Sarah Walsh (Consultant Dermatologist - KCH), Dr Catherine Smith (Consultant Dermatologist – GSTT), Karina Jackson (Consultant Nurse – GSTT), Arlene McGuire, Sheena Castelino (Dermatology Pharmacists – GSTT), Charlotte Bell (Dermatology Pharmacist – KCH), Dr Naomi Kemp (GPwSI – Southwark) and Dr Di Aitken (GP – Lambeth). The images in this guideline have been reproduced with the permission of the Primary Care Dermatology Society (PCDS). Follow up Arrangements Arrange follow up after 6-8 weeks then every 3-4 months to review the effectiveness and tolerability of treatment, as well as compliance with regimens. Advise the person to return sooner if the acne deteriorates significantly despite treatment. What Should I do if there is failure to respond to treatment? - Expect 60% improvement in 6-10 weeks and 80% by 4-6 months (slower response seen in men, severe disease, truncal acne, younger patients, seborrhoea) For patients using TOPICAL TREATMENTS in MILD, MODERATE or SEVERE ACNE: ensure that they are applying the topical to the whole area rather than individual spots CHECK ADHERENCE - poor adherence may be due to poor tolerance to treatment and is significantly worse in young males, smokers, alcoholics and those with depression, consider: a) Using a different formulation of drug (for example a cream instead of a gel; or a product which does not contain alcohol). b) Reducing the strength (for example, reducing from 10% to 5% BZPO if available). c) Switching to an alternative topical drug that causes less irritation e.g. azelaic acid or; a topical antibiotic as part of combination therapy (to reduce risk of antibiotic resistance). d) Consider adding an oral antibiotic (avoid tetracyclines in patients under 12 years of age or if pregnant/ planning a pregnancy/ breastfeeding) If adherence is adequate, consider: a) Increasing the drug strength and/or frequency of application. b) Combining different topical products (if not already doing so). Benzoyl peroxide combined with erythromycin or clindamycin is particularly effective against both non-inflammatory and inflammatory acne. For patients taking an ORAL ANTIBIOTIC in MODERATE ACNE: bear in mind that it can take up to 3 months for a response to occur: CHECK ADHERENCE a) If there has been some response, continue treatment and ensure patient is using topical BZPO or a topical retinoid or prescribe both of these as a fixed dose product. b) Consider early referral for specialist advice if there has been no response despite good compliance with oral antibiotics and topical treatments in combination and COCP in women. In SEVERE acne (especially in Type V and VI skin), refer early and initiate treatment (see below). If there is deterioration whilst waiting for referral seek advice or an urgent appointment (telephone SPR) When Should I refer a patient? Patient with features that make the diagnosis uncertain Moderate acne: patient with an inadequate response/ appearance of new lesions despite treatment with at least two oral antibiotics PLUS topical treatments, each given for at least 3 months (especially in individuals with type V/VI skin with associated hyperpigmentation) or patients who are developing scarring, or are at risk of developing it, despite primary care interventions. Severe acne : Refer early: patients with painful, deep, nodules or cysts (nodulocystic acne), scarring acne, patient with a severe variant of acne with systemic symptoms such as acne fulminans (urgent referral) or patient who is unwell with flu-like symptoms and myalgia with nodulocystic acne (discuss with on call SpR) When considering referral to secondary care Dermatology services a) Lambeth patients ONLY: please use the Acne vulgaris referral form where appropriate b) Southwark patients ONLY: please review the acne checklist before referral to the Southwark Community Dermatology Service including details of acne severity & prior treatment. Consider routine referral for female patients suspected of having an underlying endocrinological cause of severe and recalcitrant acne with features of masculinisation (such as severe polycystic ovary syndrome) requiring assessment e.g. Free testosterone >5 nmol/L Consider an urgent referral to secondary care for patients with acne who have severe psychosocial problems, for example a morbid fear of deformity (body dysmorphic disorder), or people who have suicidal ideation (likely to achieve better outcome), likely to require input from dermatology AND psychological medicine/liaison psychiatry.
- 3. Management of Acne - Key Prescribing and Counselling information for Healthcare Professionals • Check for acne inducing medication e.g. lithium, ciclosporin, topical or anabolic steroids, vitamin B12 injections (this is NOT an exhaustive list) & ensure patient is not using comedogenic (greasy) emollients/ hair preparations. • Patients who have Fitzpatrick scale type V/VI skin (Asian/African/Afro-Caribbean) are more prone to hyperpigmentation - consider treating as though acne were at a more severe stage. To improve compliance with topical preparations encourage patients to test a small amount on inside of forearm once daily for 5 days, then leave on face just for a couple of hours or use on alternate days before progressing to overnight applications. Treat whole area not just existing spots. • Prescribe gels for greasy skin, creams for dry skin; use keratolytics at night as inflammatory response will fade by the morning. • Give patient information leaflet http://www.patient.co.uk/health/Acne.htm to improve understanding and compliance • Images to guide prescribing are available at http://www.pcds.org.uk/clinical-guidance/acne-vulgaris#images Benzoyl peroxide (BZPO): has keratolytic and antimicrobial properties; it can bleach bedding and clothing. lower concentrations seem to be as effective as higher concentration; start low and increase concentration gradually counsel patient to apply at night, there will be local skin irritation upon initiation but scaling and redness will often subside with treatment; if troublesome, consider reducing application frequency or suspend until irritation subsides and reintroduce at a reduced application frequency Avoid excessive exposure to sunlight. Some forms of BZPO are available to purchase ‘Over the Counter’ and have a lower acquisition cost than a prescription. Topical retinoids: have anticomedonal properties; several months of treatment may be required to achieve optimal response; continue treatment until no new lesions develop counsel patient redness and skin peeling can occur initially but will often subside with treatment; if troublesome consider reducing application frequency or suspend until irritation subsides and reintroduce at reduced application frequency avoid use in severe acne over large areas; avoid exposure to UV light or if unavoidable use appropriate sunscreen and protective clothing are contraindicated in pregnancy; counsel women of child bearing age to use effective contraception (oral progestogen only contraceptives not indicated as may worsen acne ). Azelaic acid: has antimicrobial and anticomedonal properties; is considered less likely to cause local irritation than BZPO therefore may be an alternative in facial acne; can cause skin lightening in type VI skin Topical antibacterials: can cause mild skin irritation, rarely sensitisation and GI disturbances reported with topical clindamycin; antibacterial resistance to P.acnes is increasing therefore to avoid development of resistance use antimicrobial preparations such as benzoyl peroxide or azelaic acid at the same time. avoid concomitant treatment with oral and topical antibacterials (to reduce anti-microbial drug resistance); can be useful in patients wanting to avoid systemic antibiotics; treatment with topical antibacterials should be continued for at least 6 months but do not continue for longer than necessary Systemic antibiotics: Tetracyclines are contra-indicated in pregnancy and patients under 12 years of age; erythromycin may be a suitable alternative for these patients. Absorption of tetracyclines is affected by antacids. Prescribing topical adapalene, fixed dose adapalene with benzoyl peroxide or azelaic acid with oral antibiotics reduces the development of resistant strains of P acne There is a lack of evidence to suggest one tetracycline is superior to another in terms of efficacy. Once daily preparations which can be taken with food and plenty of water, may reduce nausea and aid compliance (especially in teenagers). Doxycycline may cause more photosensitivity than lymecycline especially in higher doses and fair skinned individuals. Use of non-comedogenic sunscreens may prevent this. If photosensitivity occurs with doxycycline, consider switching to lymecycline. Minocycline is no longer considered a first line therapy due to associated serious ADRS Once patients have had a sustained improvement to systemic treatment (at least 3 months) consider discontinuing and continue to manage with topical treatments. For women wanting contraception or whose moderate papulo-pustular acne is not improving after 3/12 of oral antibiotics and topical keratolytic; a low acquisition cost COCP (especially those containing levonorgestrel) may be effective. Co-cyprindiol: is especially suitable for women with PCOS/ hirsutism, for those with moderate nodular or severe acne and 2 nd line if not improving after 3/12 of standard COCP, oral antibiotics and topical keratolytic. Preparations containing abrasive agents: such as aluminium oxide or nicotinamide are considered less effective treatments. Oral isotretinoin: only to be initiated and prescribed by a consultant dermatologist due to the serious side effects including teratogenic and possible psychiatric effects; ensure women are using effective contraception prior to referral. NHS Lambeth CCG and NHS Southwark CCG Guidelines for the Management of Acne. Approved by: Lambeth and Southwark Joint Prescribing Committee Date: Feb 2014 Review date: Feb 2016 Direct any queries to: LAMCCG.medicinesoptimisation@nhs.net 0203 049 4197 or SOUCCG.medicines-optimisation@nhs.net 0207 525 3253 Page 3 of 4
- 4. Primary and Secondary Care Prescribing Formulary Product Dose Advice/Restrictions for prescribing (For full prescribing information please refer to BNF Online or Summary of Product Characteristics) Cost (Drug Tariff & MIMs Online Dec 14) Topical preparations Benzoyl peroxide gel 5% (Acnecide) 1-2 x daily Good for patients with greasy skin; once daily application; can bleach towels, clothes and bedding. 30g = £5.44† Benzoyl peroxide cream 5% OD night Good for patients with dry skin; can bleach towels, clothes and bedding. 40g = £1.89 Benzoyl peroxide cream 10% 2-3 x daily Good for patients with dry skin; can bleach towels, clothes and bedding. 50g = £4.59 Benzoyl peroxide cream 4% 1-2 x daily Good for patients with dry skin; can bleach towels, clothes and bedding. 50g = £4.13 Benzoyl peroxide 5% + clindamycin phosphate 1% Gel OD night Good for patients with greasy skin 25g = £10.94† Benzoyl peroxide 3% + clindamycin phosphate 1% Gel OD night Good for patients with greasy skin and when patient is experiencing sensitivity with 5% strength product 30g = £11.94 Azelaic acid 20% cream 1-2 x daily 30g = £3.74 Erythromycin/Zinc acetate lotion 40mg/ml/12mg/ml 2 x daily Reconstituted with ethanol based solvent; good for patients with greasy skin 30ml = £7.71† Clindamycin phosphate topical solution 1% OD Sponge applicator - aqueous alcoholic basis; for greasy skin 30ml = £4.34† Clindamycin phosphate lotion 1% OD Roll-on applicator - aqueous basis; for dry skin 30ml = £5.08† Clindamycin phosphate gel 1% OD Good for patients with greasy skin 30g = £8.66 Erythromycin topical solution 2% BD Alcoholic basis; good for patients with greasy skin 50ml = £7.69 Adapalene 0.1% cream OD Contraindicated in pregnancy; good for patients with dry skin 45g = £16.43 Adapalene 0.1% gel OD Contraindicated in pregnancy; good for patients with greasy skin 45g = £16.43 Isotretinoin 0.05% gel OD Contraindicated in pregnancy; good for patients with greasy skin 30g = £5.94 Adapalene 0.1%+ benzoyl peroxide 2.5% gel OD night Contraindicated in pregnancy; may need to apply a non-comedogenic moisturiser 45g = £17.91 Isotretinoin 0.05% + erythromycin 2% gel OD night Contraindicated in pregnancy 30g = £7.47 Tretinoin 0.025% + erythromycin 4% solution 1-2 x daily Contraindicated in pregnancy; alcoholic base 25ml = £7.05 Systemic preparations (Tetracyclines are contraindicated in pregnancy and children under 12 years of age) Doxycycline 100mg capsule 100mg OD 1st line choice; take with food and plenty of water to reduce nausea; use sunscreens with sunshine exposure, to minimise photosensitivity 28 = £3.99 Lymecycline 408mg capsule 408mg OD Alternative 1st line choice especially in patients experiencing photosensitivity/ ADRs/ contraindication/ intolerance/ inefficacy with doxycycline 28 = £8.74 Oxytetracycline 250mg tablet 500mg BD Alternative choice; if patient can take 1 hour before or 2 hours after food 112= £4.88 (28/7) Erythromycin 250mg gastro-resistant tablets 500mg BD For use IN PREGNANCY or contraindication/intolerance to tetracyclines 112 = £ 7.56 (28/7) Trimethoprim 100mg, 200mg tablet As advised UNLICENSED USE; Specialist initiation only (GPwSI/Consultant): For moderate-severe resistant acne where topical treatment & systemic antibiotic therapy are ineffective or inappropriate 28 x 200mg = £2.02 28 x 100mg =£1.08 Minocycline 100mg MR capsule As advised SECONDARY CARE INITIATION ONLY; use limited to exceptional circumstances due to risk of serious ADRs 28 = £10.04 Combined oral contraceptive pill As advised Consider the lower acquisition cost COCPs first line Co-cyprindiol 2000/35 tablets 1 OD WOMEN ONLY, moderate nodular or severe acne or as 2nd line - see BNF online for CSM warning 63 = £5.42 Isotretinoin 10mg and 20mg capsules As advised SECONDARY CARE INITIATION AND PRESCRIBING ONLY 30 x10mg = £14.54 30 x 20mg = £19.55 Cyproterone acetate tablet As advised Specialist initiation - severe or resistant acne in women only † larger pack sizes available NHS Lambeth CCG and NHS Southwark CCG Guidelines for the Management of Acne. Approved by: Lambeth and Southwark Joint Prescribing Committee Date: Feb 2014 Review date: Feb 2016 Direct any queries to: LAMCCG.medicinesoptimisation@nhs.net 0203 049 4197 or SOUCCG.medicines-management@nhs.net 0207 525 3253 Page 4 of 4