This document summarizes lichen sclerosus (LS), a chronic inflammatory skin condition that affects the vulva. It discusses the epidemiology, clinical presentation, histopathology, differential diagnosis, complications, treatment and management of LS. Key points include:
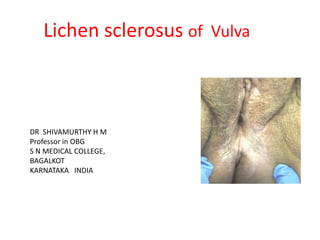
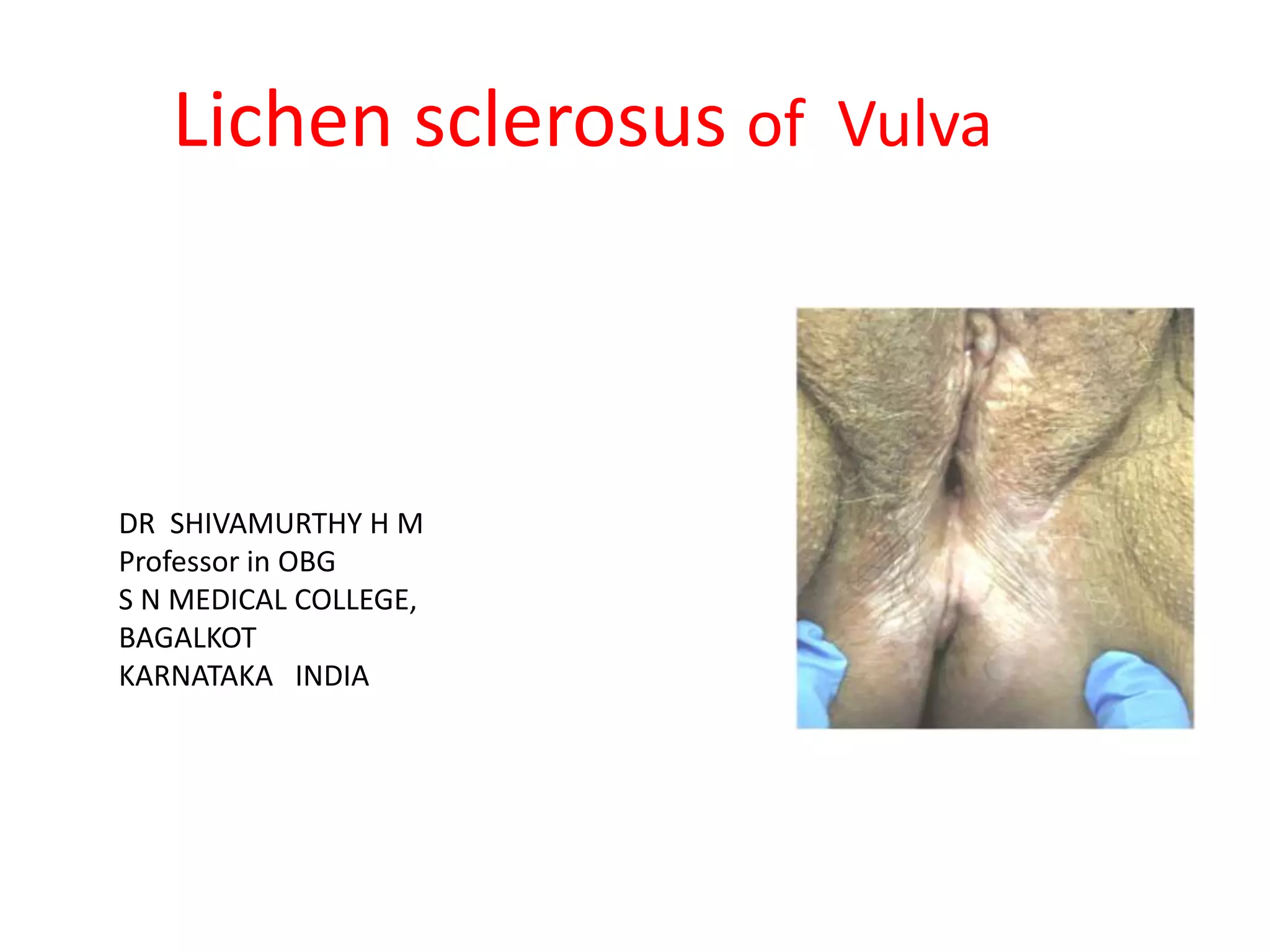
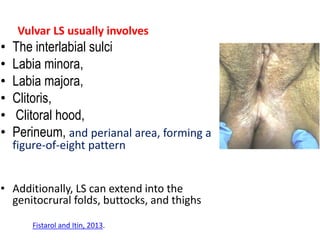
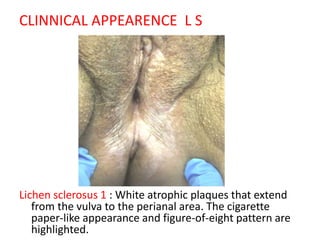
- LS typically presents as white plaques or papules in a figure-of-eight pattern around the vulva and perianal area.
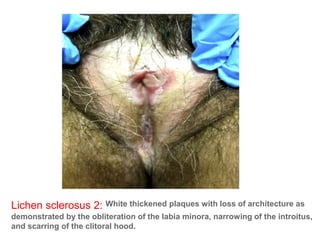
- It is a chronic condition that can cause scarring and fusion of genital tissues if left untreated. There is also an increased risk of vulvar squamous cell carcinoma.
- Ultra-potent topical corticosteroids are the first-line treatment. Long-term maintenance therapy is important to














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






