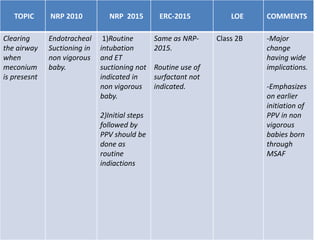
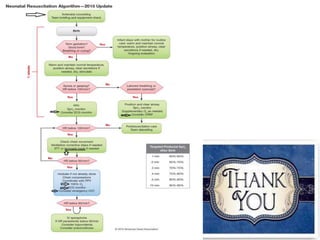
This document summarizes 2015 guidelines from the American Heart Association on resuscitation of babies born through meconium-stained amniotic fluid (MSAF). It finds that routine oropharyngeal and tracheal suctioning is not recommended for non-vigorous babies, as evidence shows it does not provide benefits and risks delaying other important resuscitation steps. For non-vigorous babies, the initial steps of resuscitation should be followed by positive pressure ventilation if needed. While an individual skilled in intubation should be present for babies with suspected fetal distress, routine intubation and suction is not suggested due to insufficient evidence of benefits and risk of harm. The guidelines emphasize early initiation of ventilation for non-