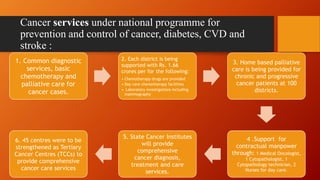
The document discusses India's National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS). It was established to address the growing burden of non-communicable diseases in India. The program merged the National Cancer Control Programme and National Diabetes Control Programme. It aims to promote healthy lifestyles, screen high-risk populations, build healthcare capacity, and strengthen tertiary care facilities. Key activities include health education, opportunistic screening, NCD clinics, and referral systems across primary, community and district levels.



















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









