Downloaded 700 times
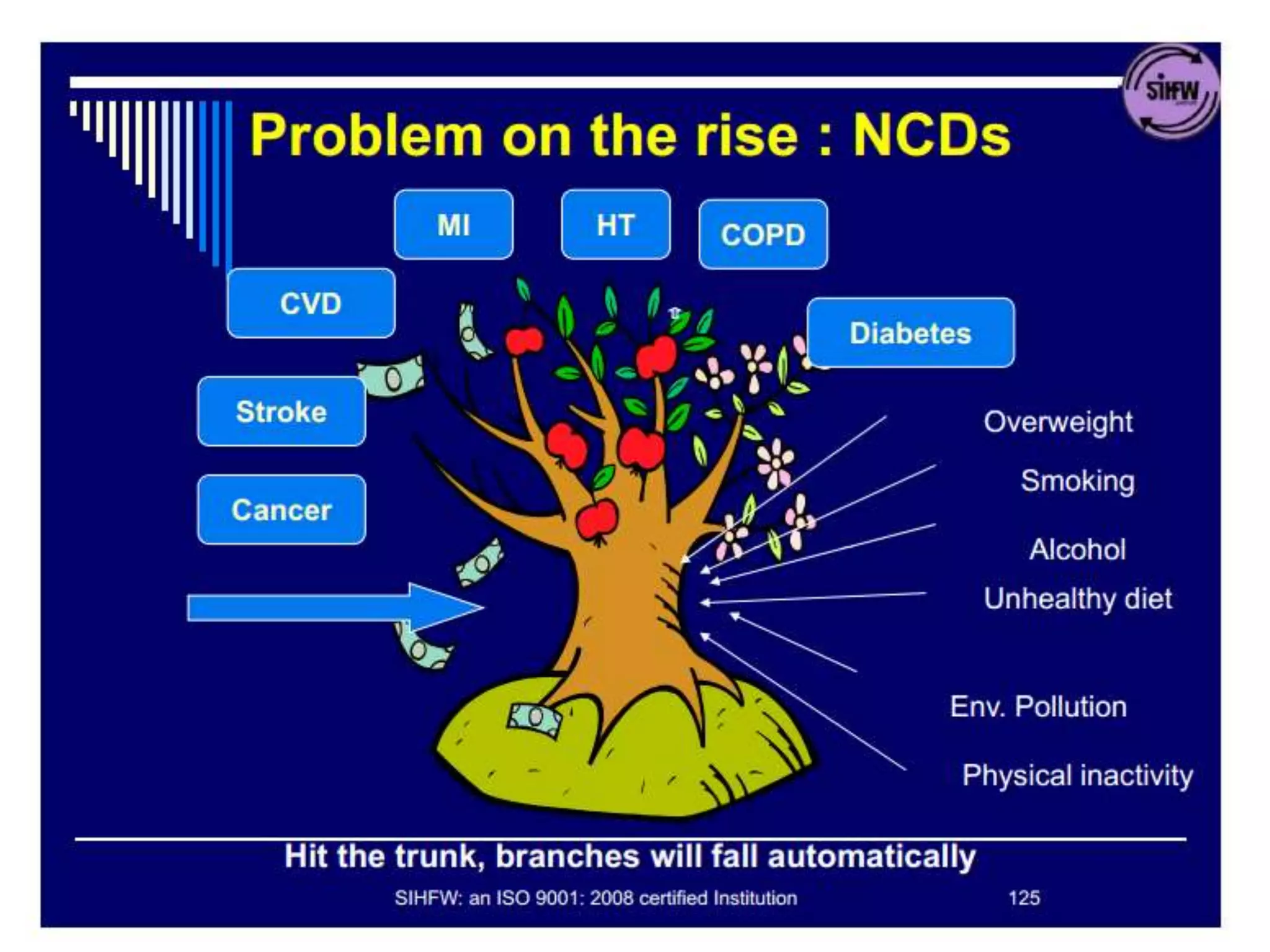
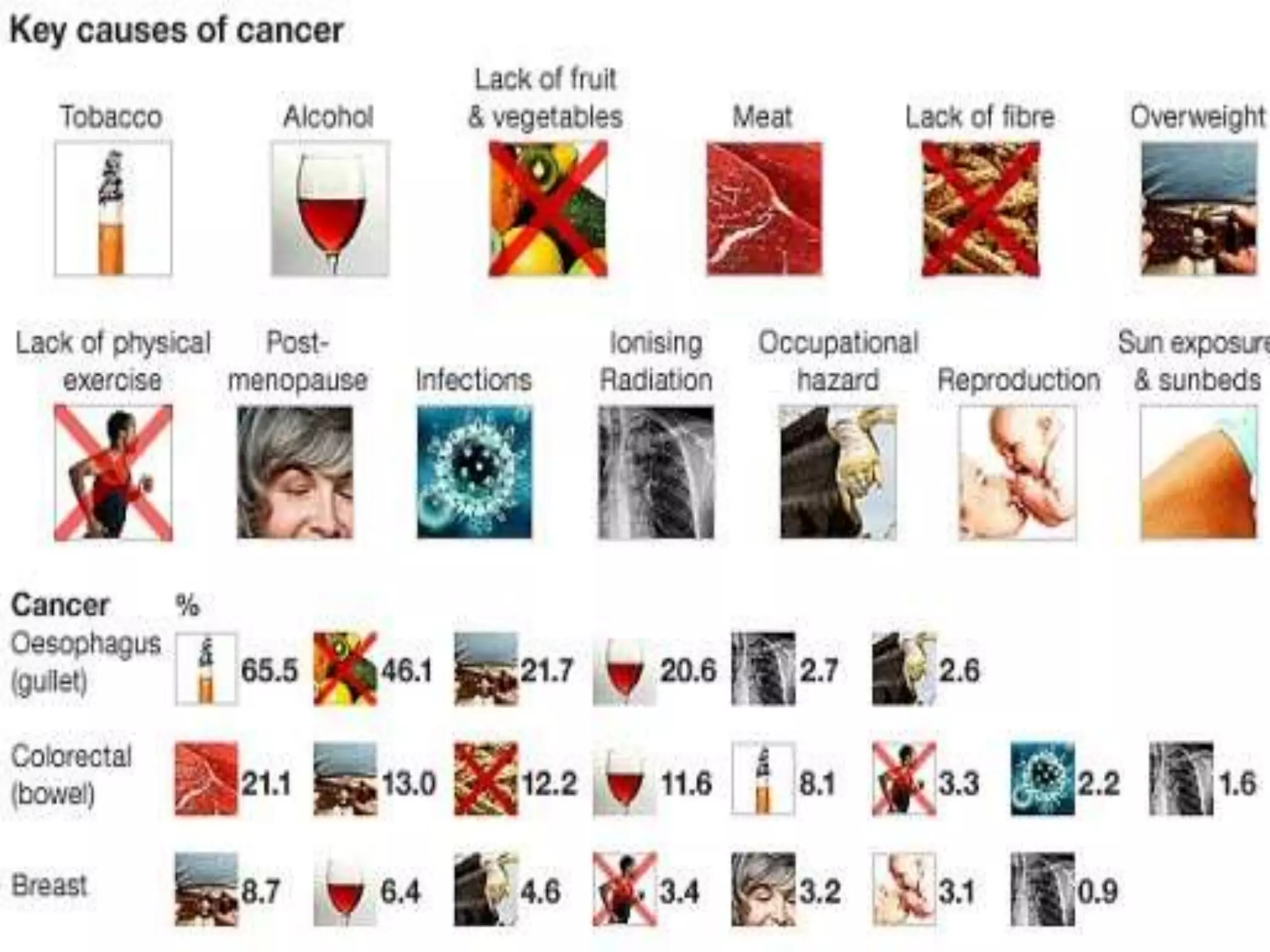
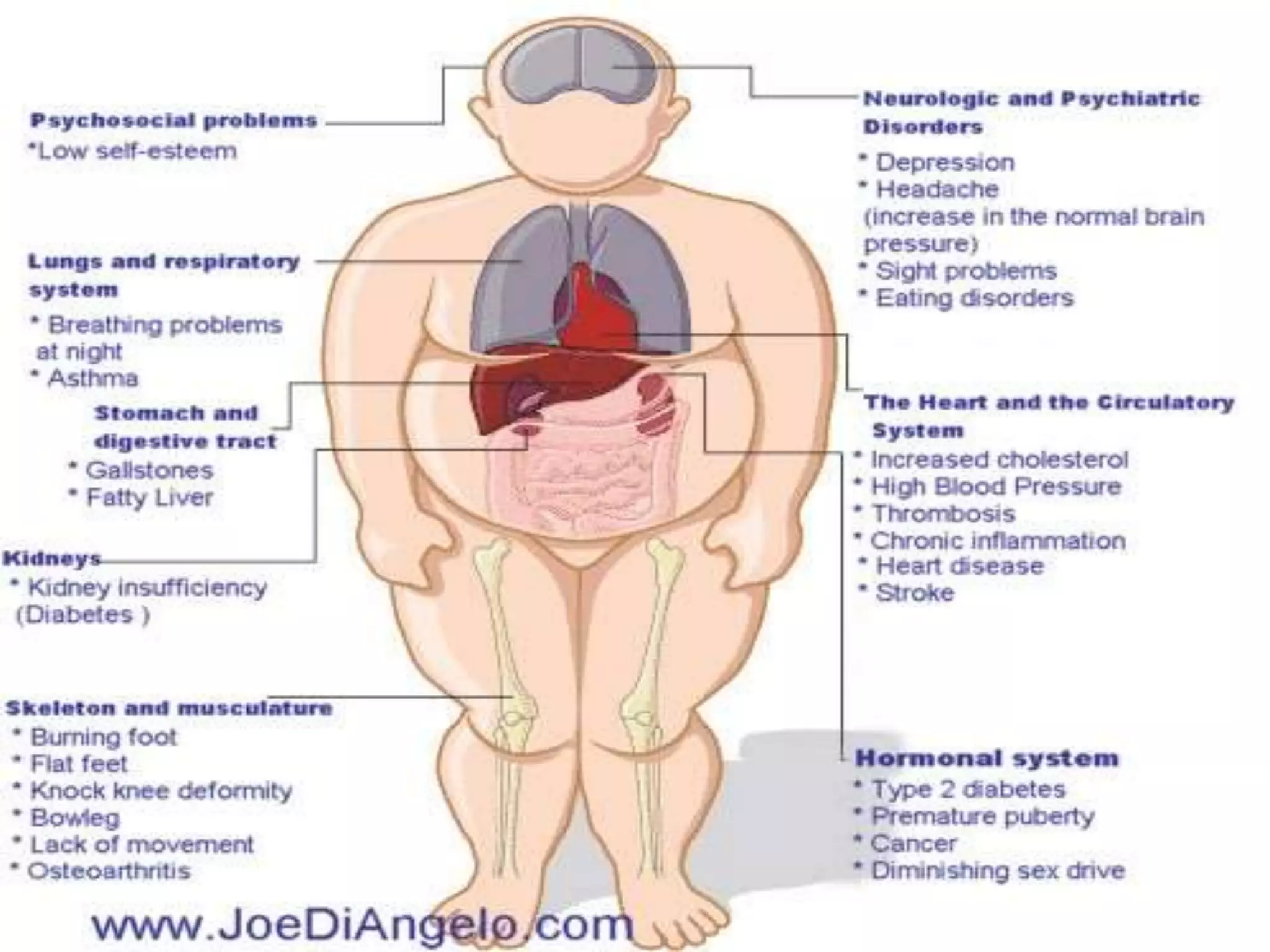
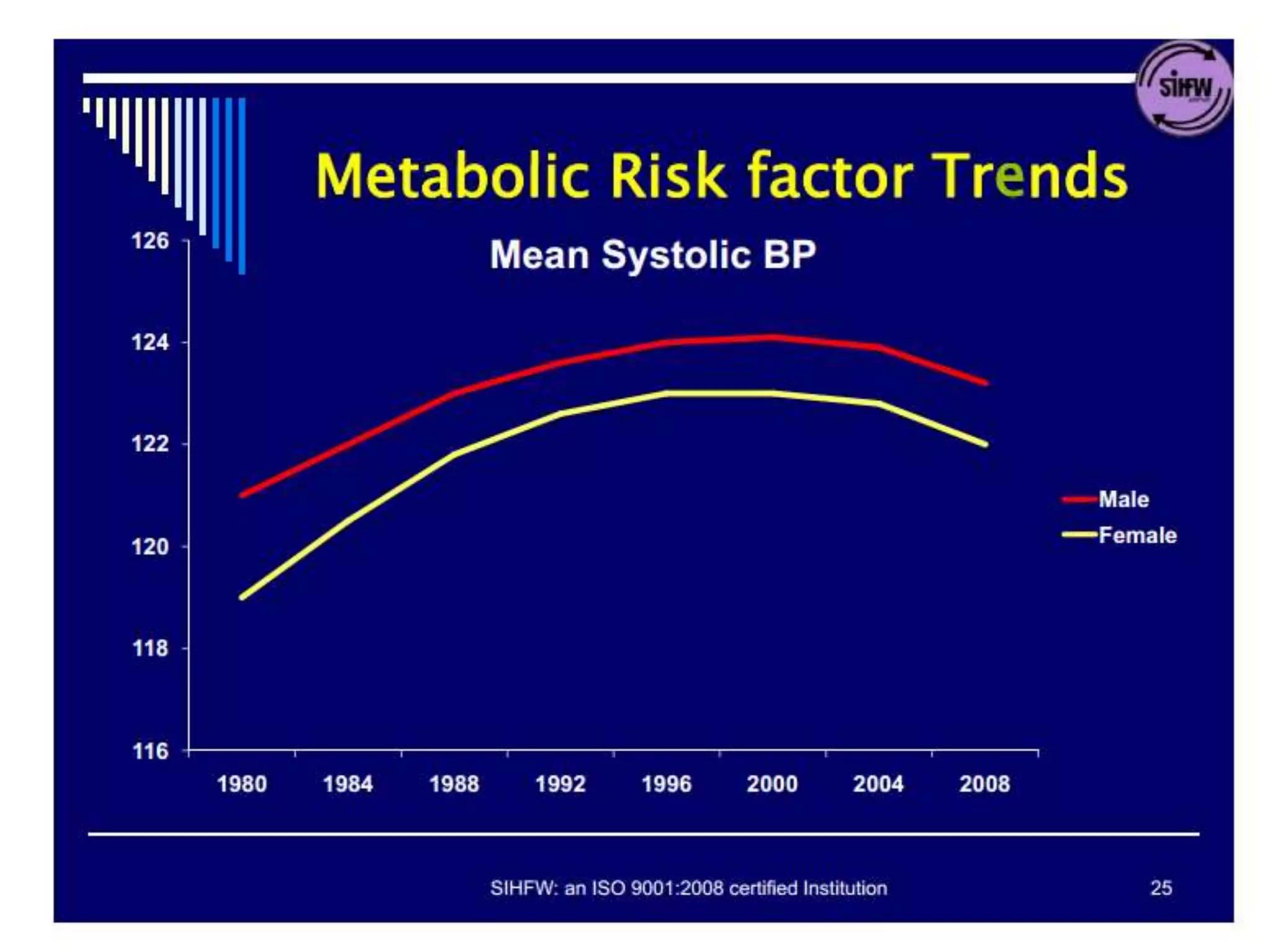
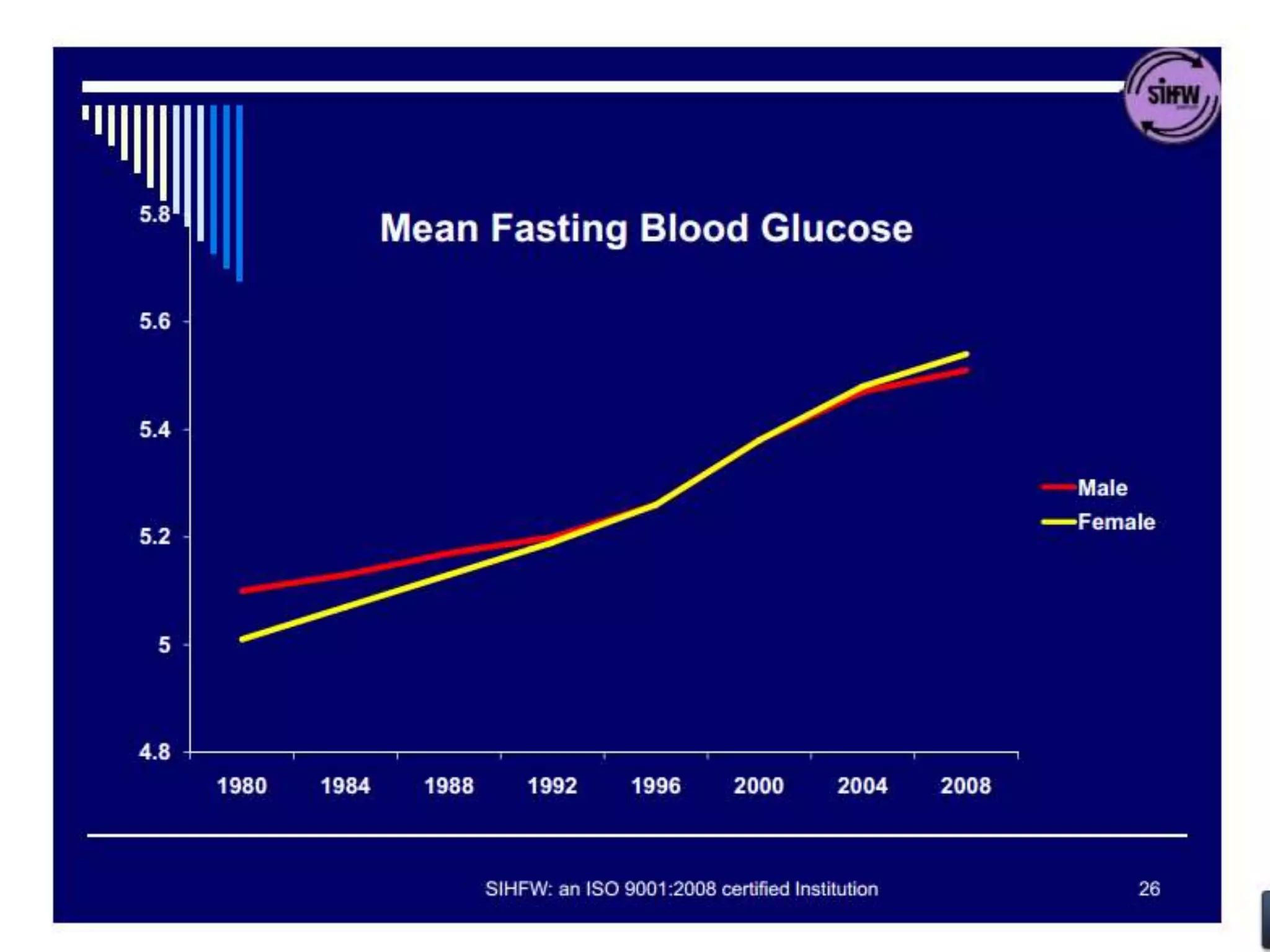
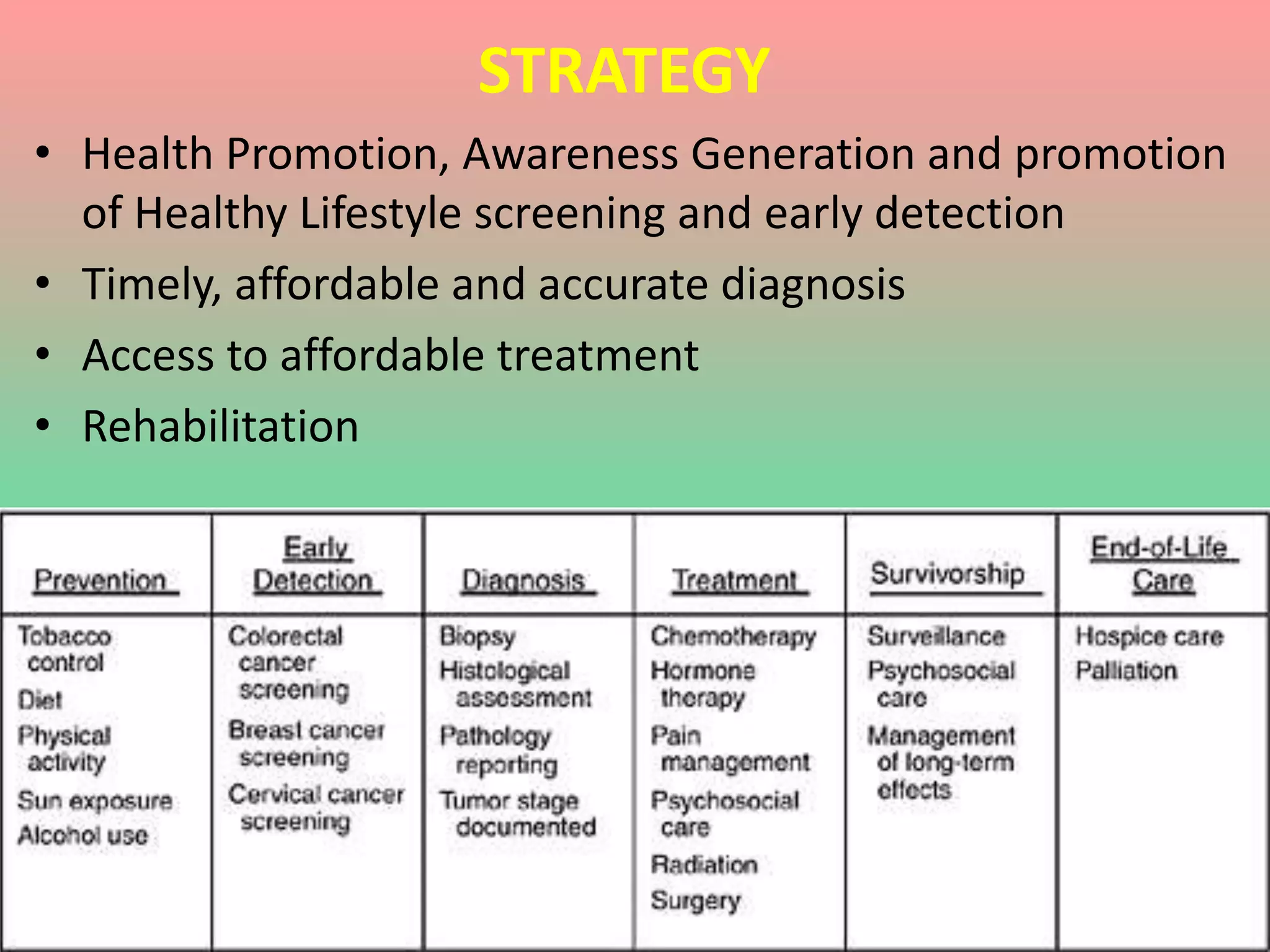
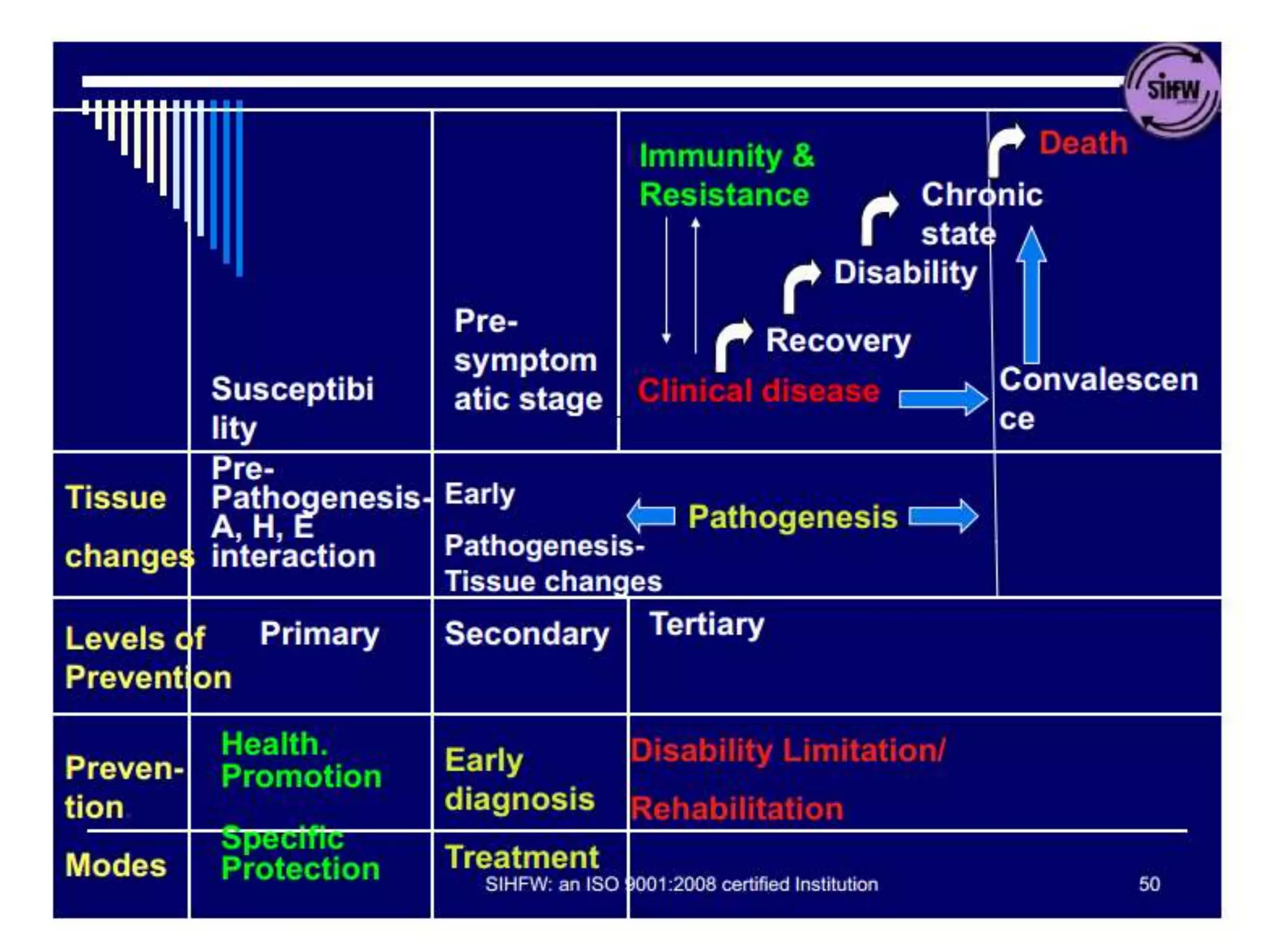
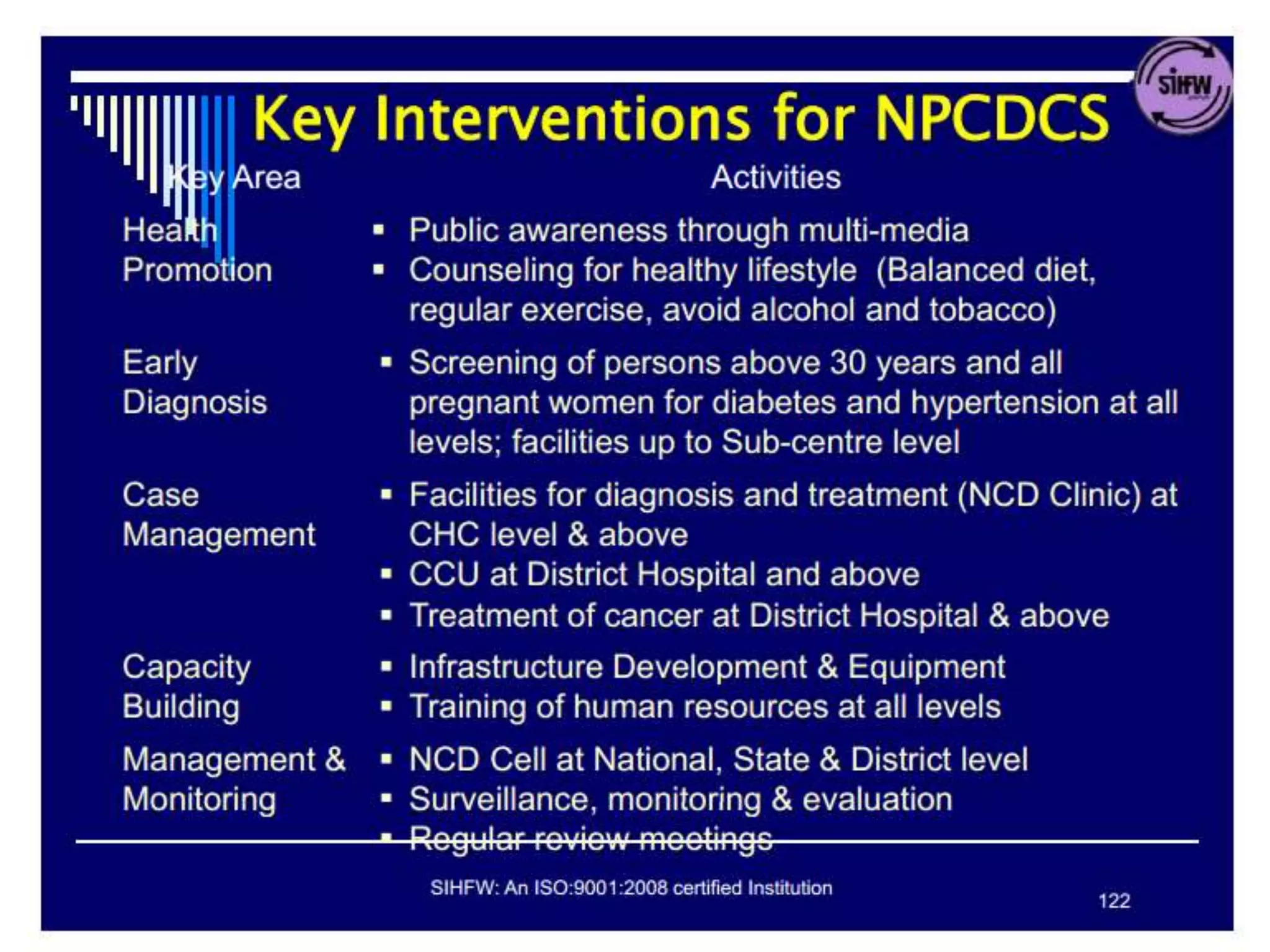


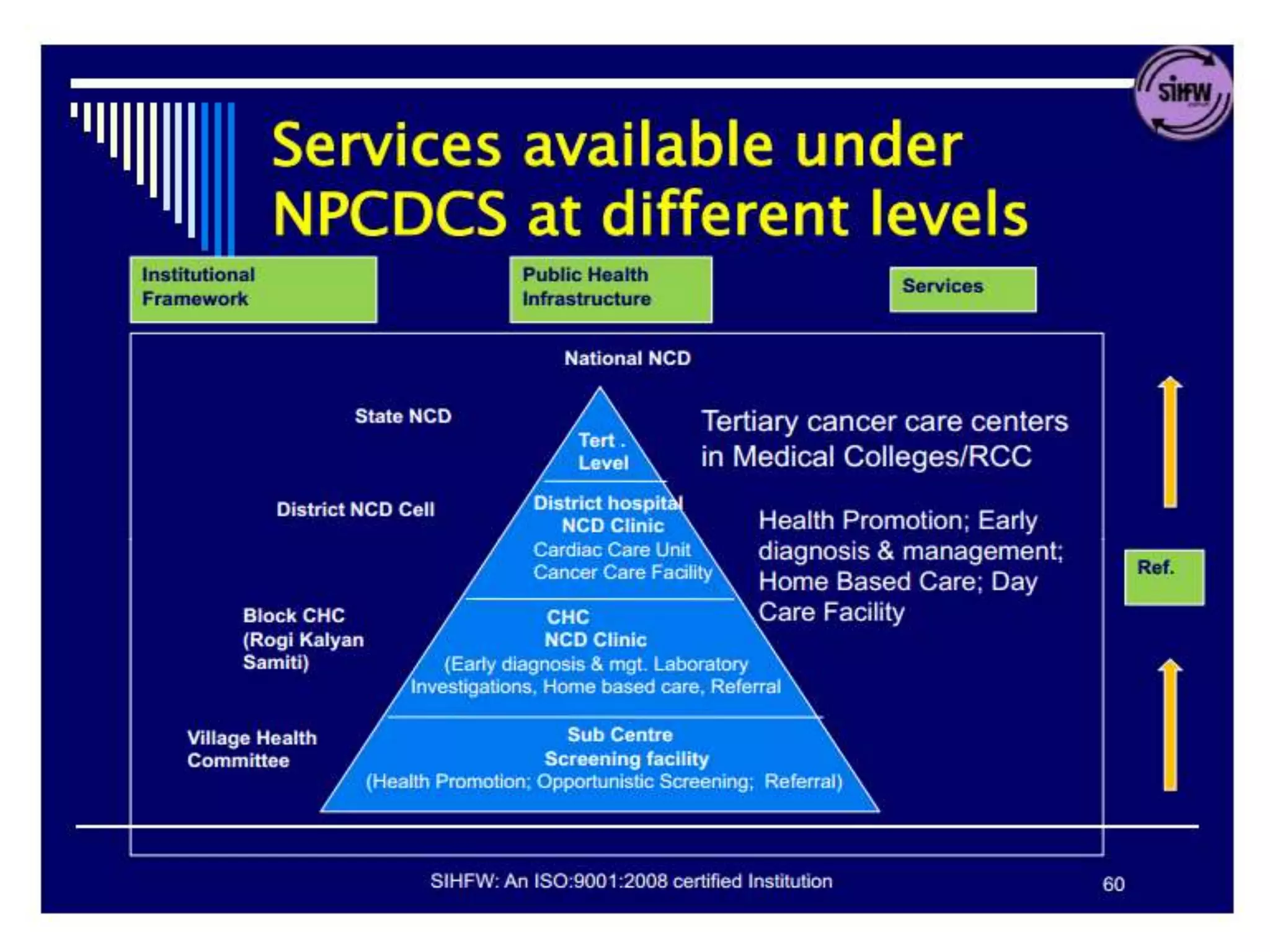
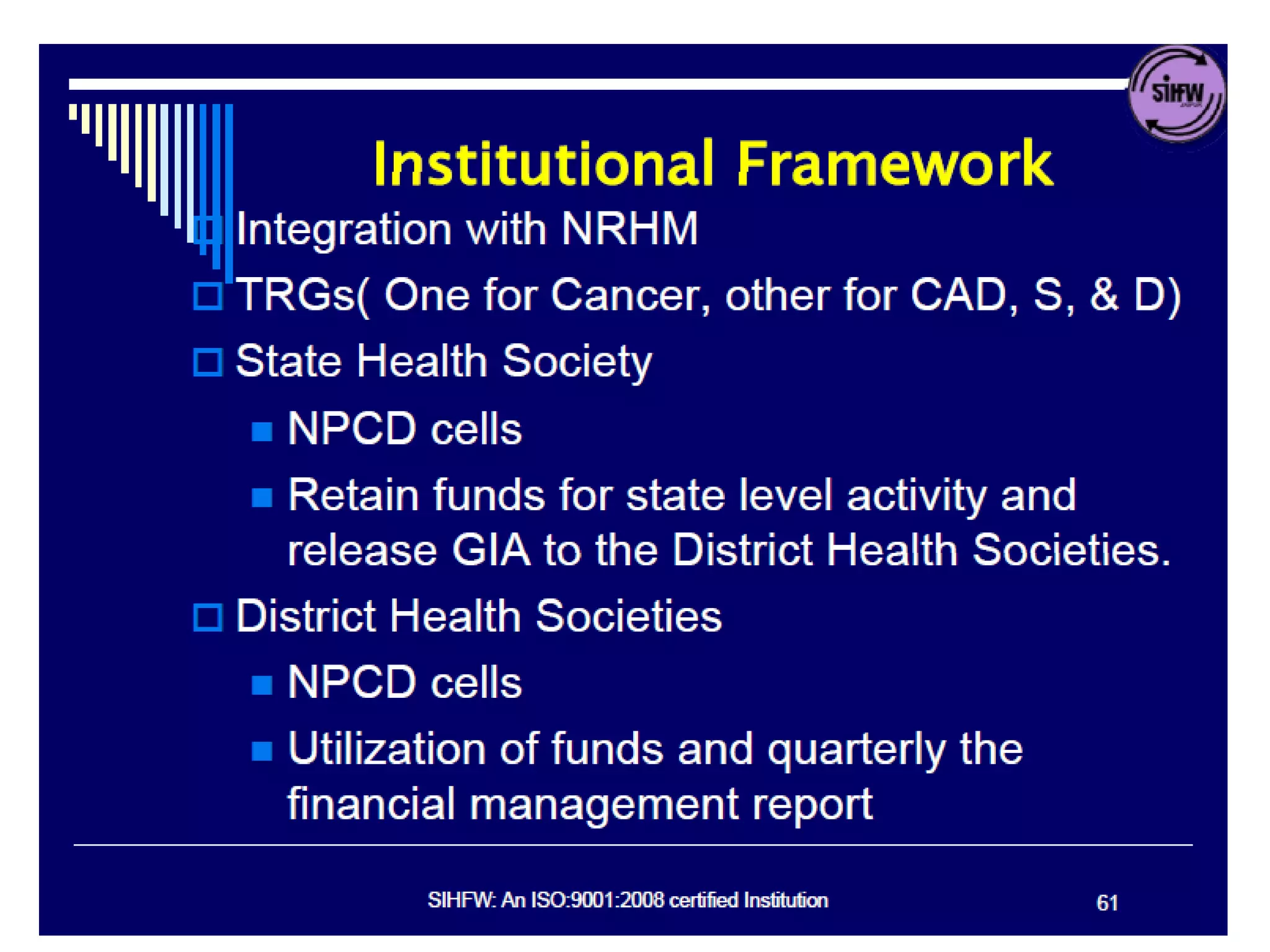
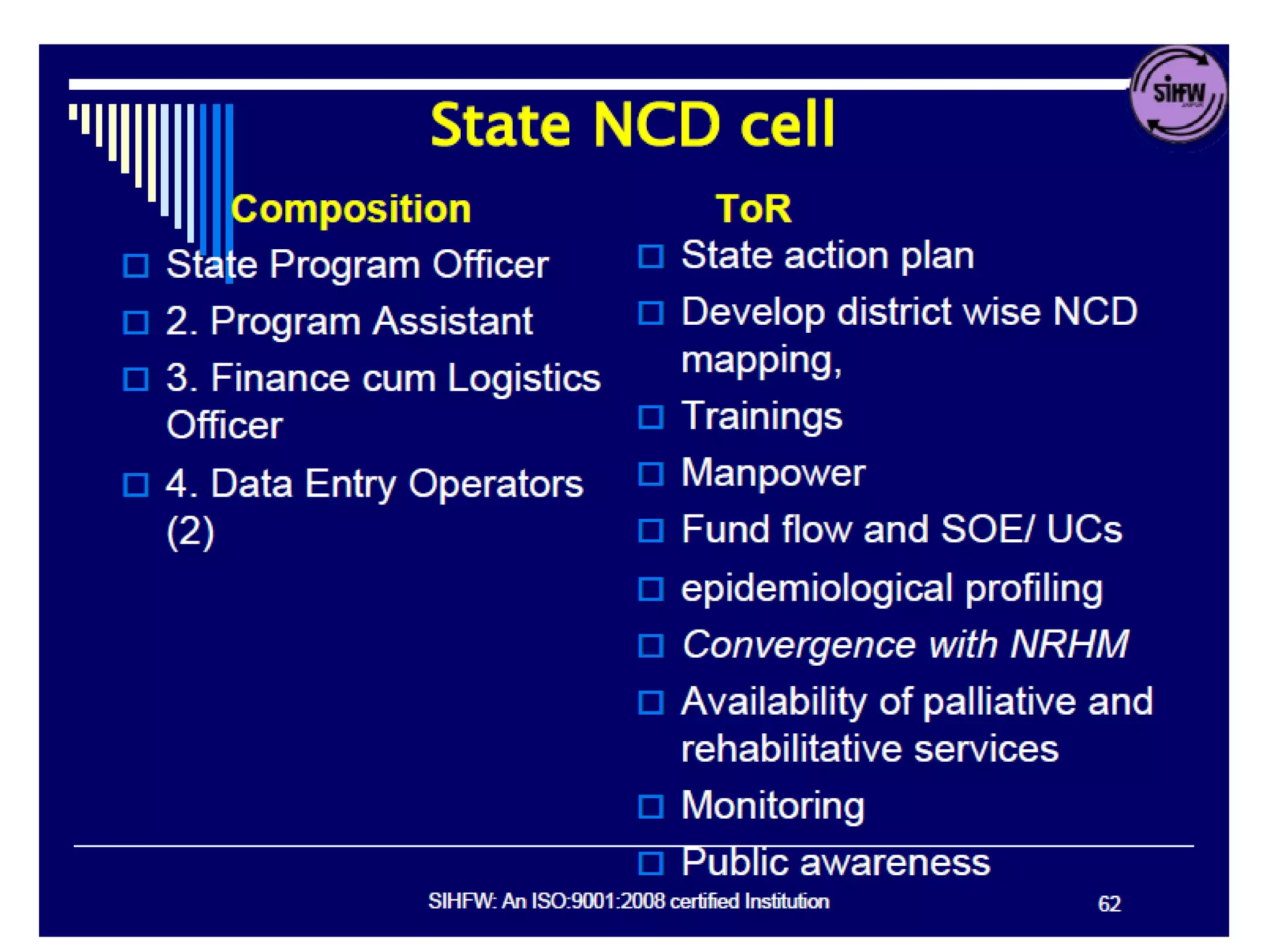
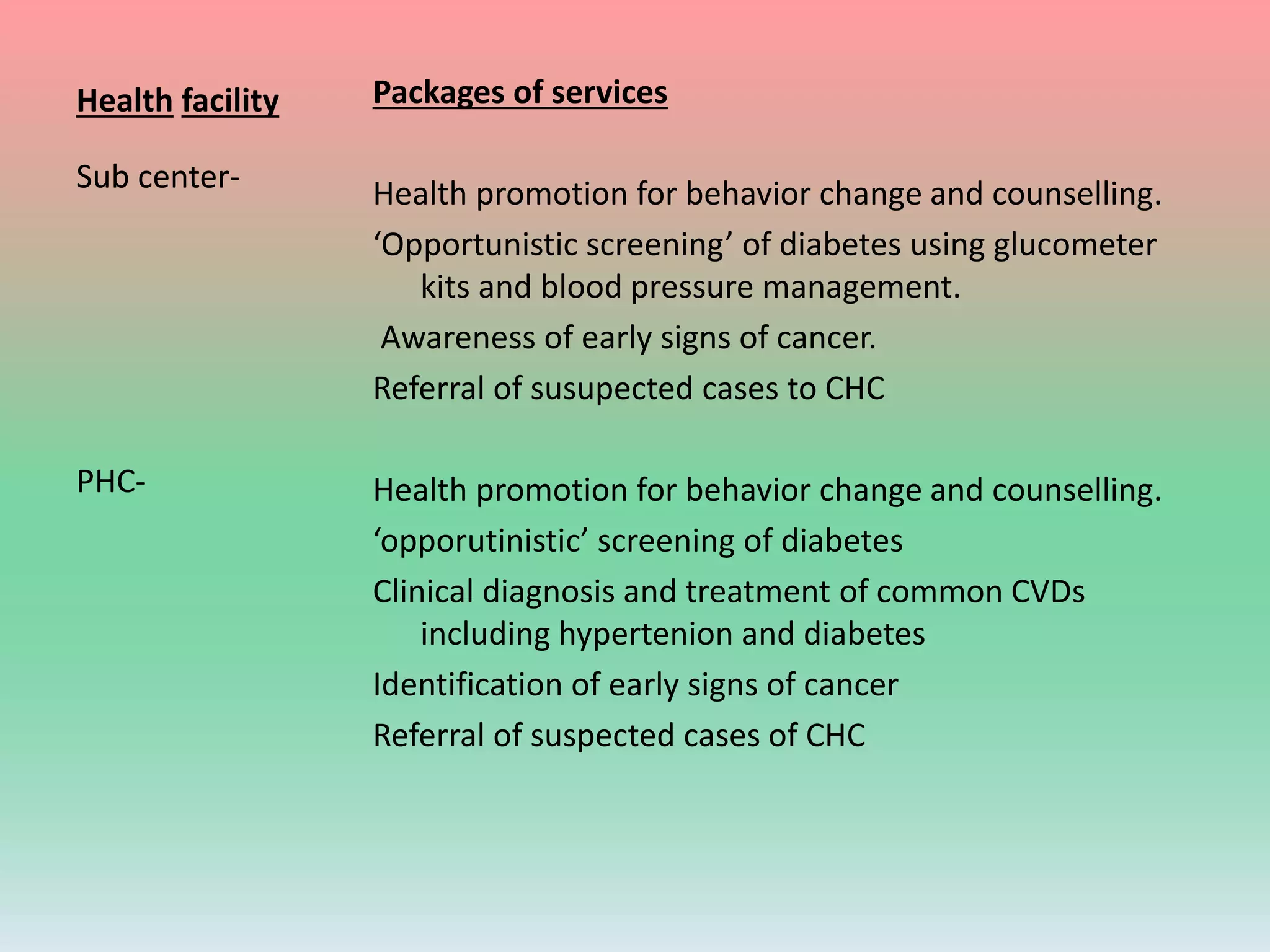
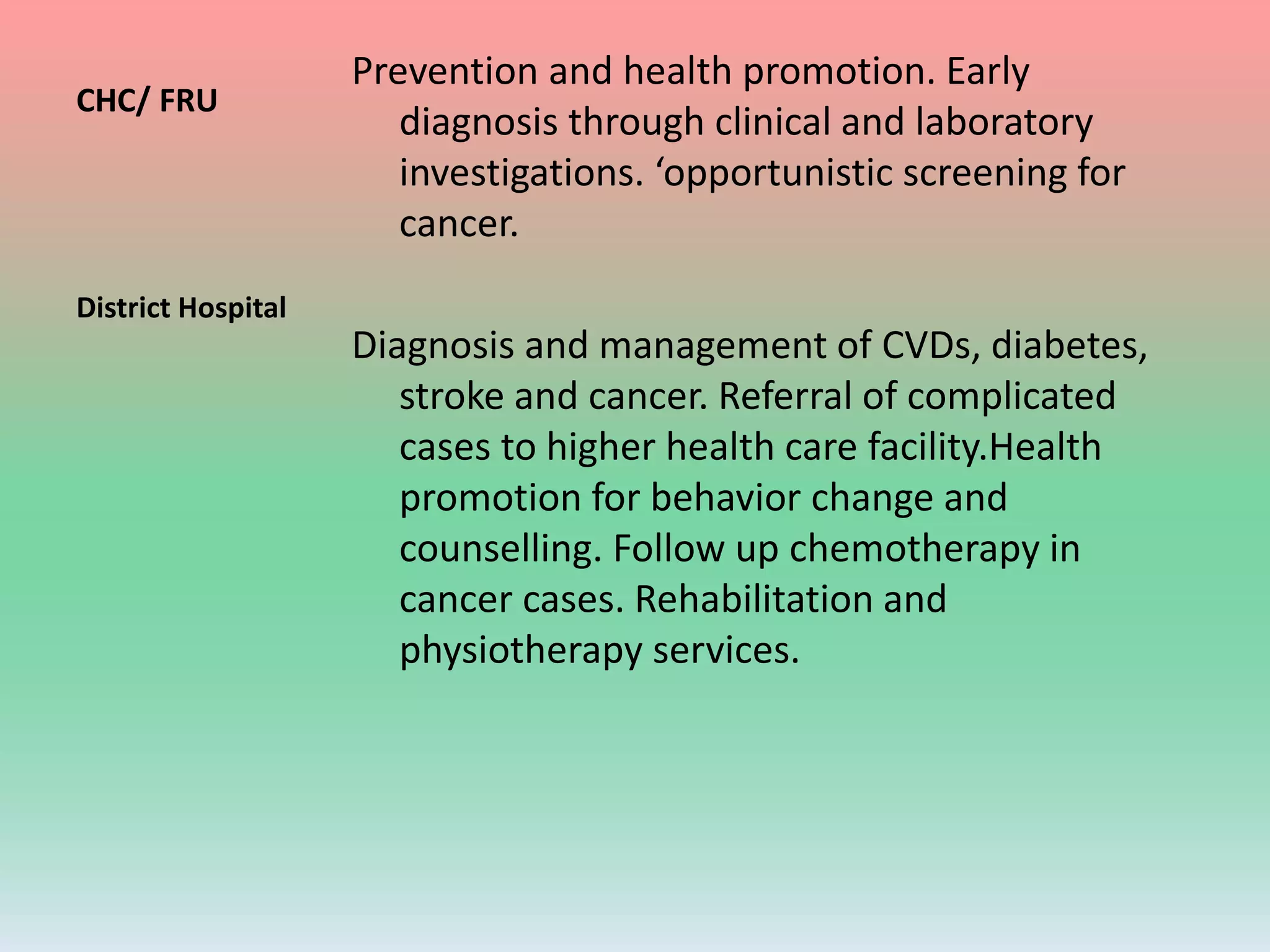
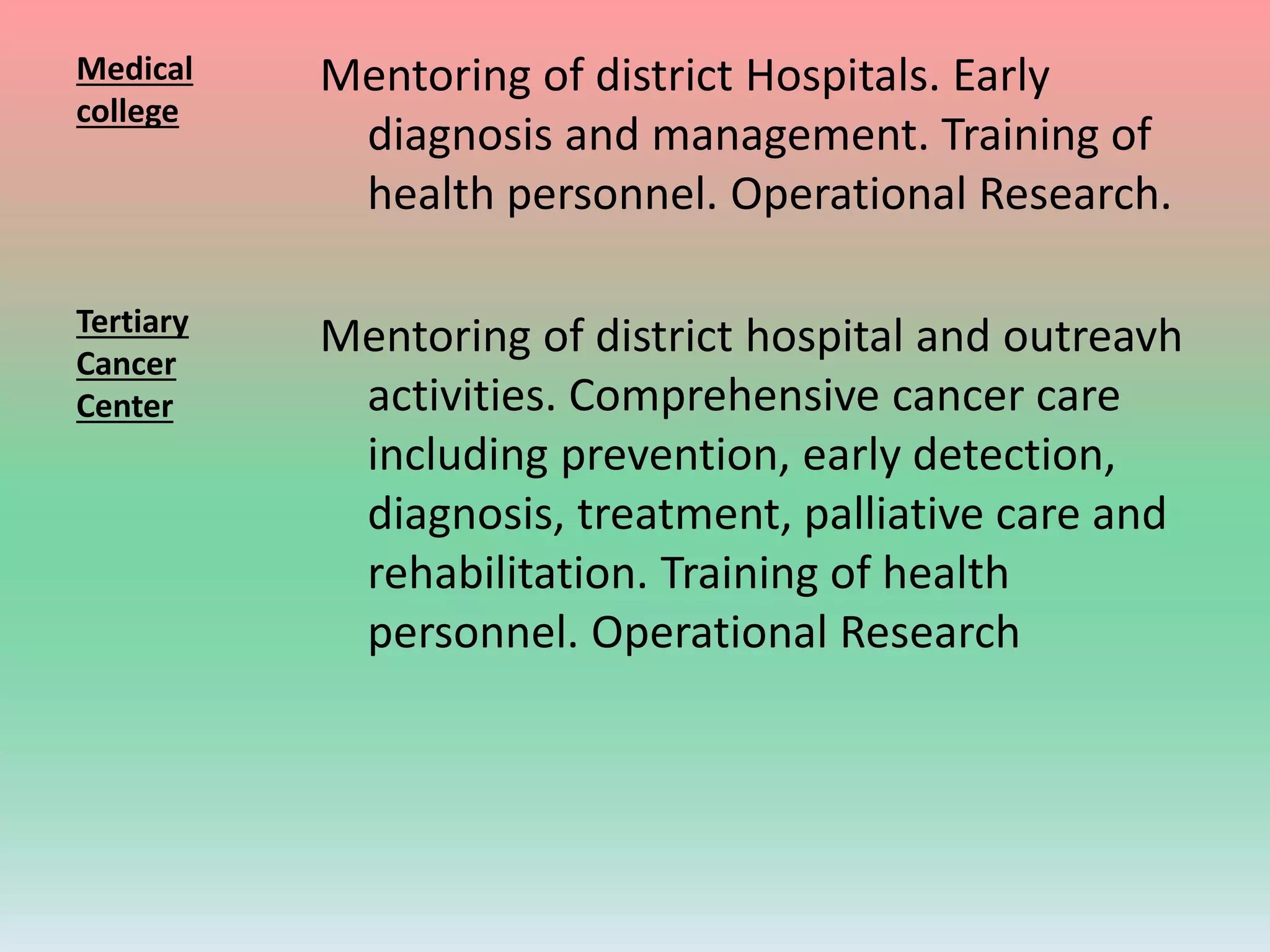

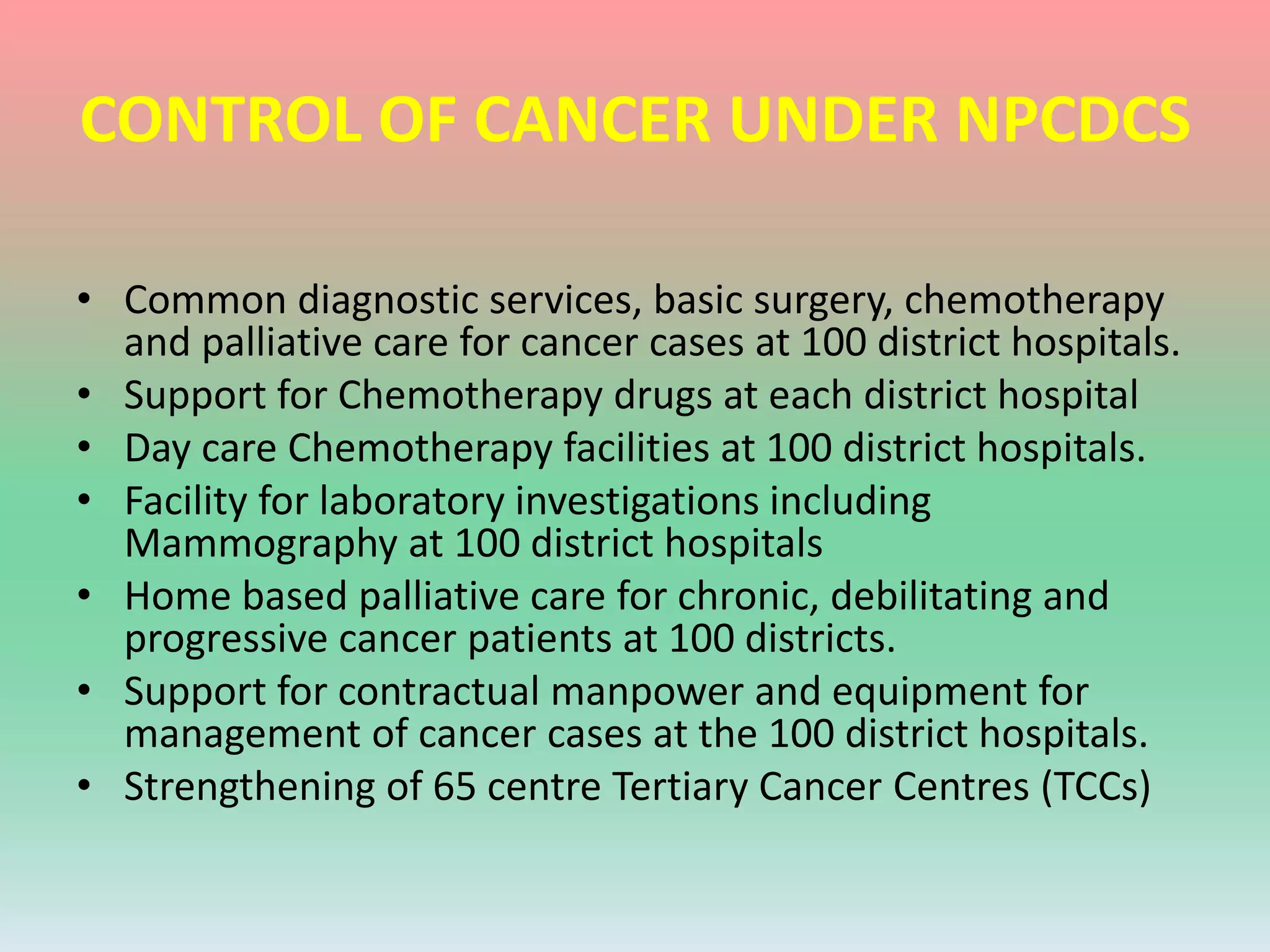
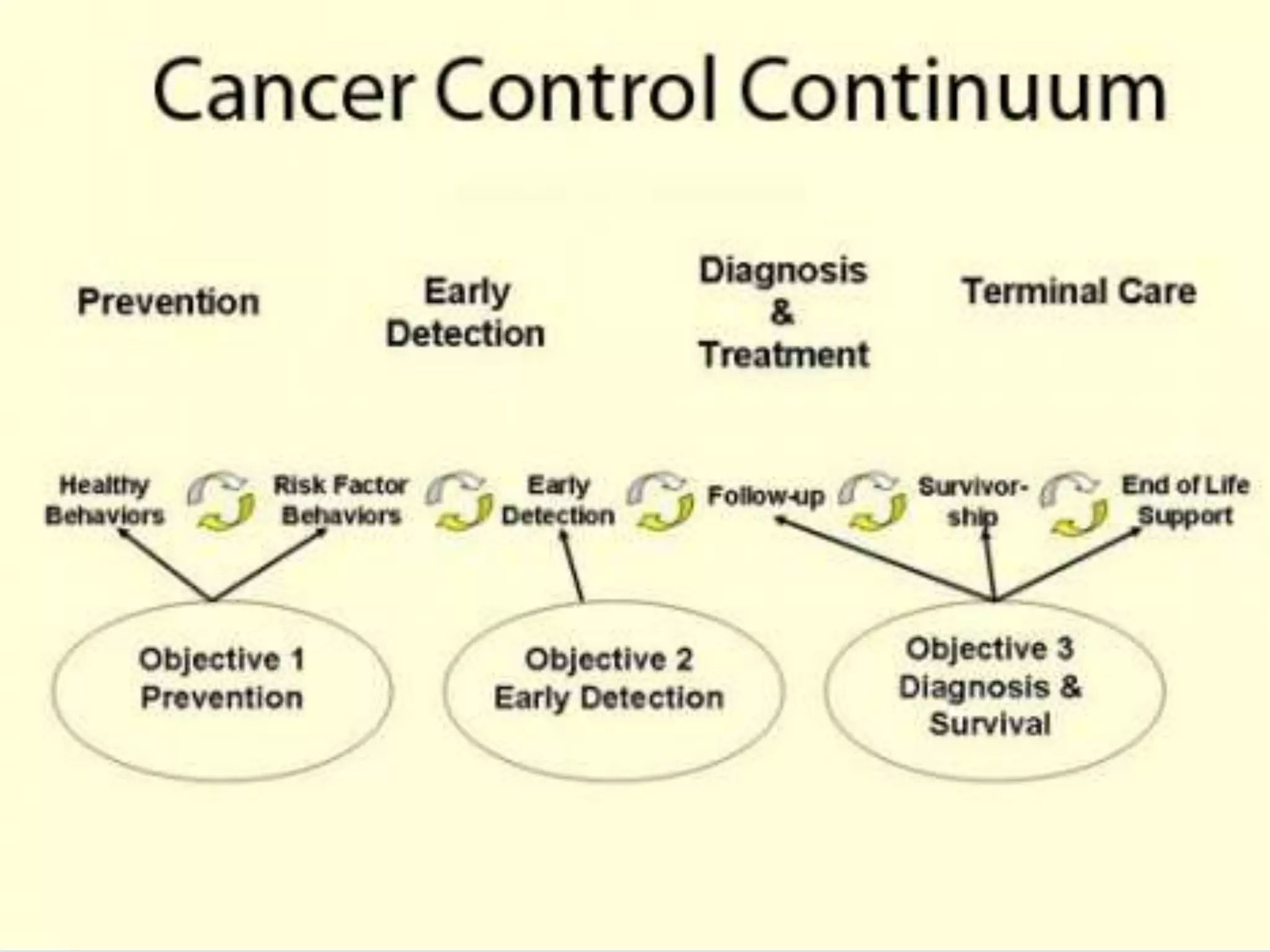

The document outlines India's National Programme for Control and Prevention of Non-Communicable Diseases (NPCDCS) such as cancer, diabetes, cardiovascular diseases and stroke. It aims to integrate NCD prevention and control with primary healthcare and improve early diagnosis, management and treatment of NCDs. Key objectives include preventing NCDs through lifestyle changes and screening, building healthcare capacity for NCDs, and improving access to treatment. The program promotes healthy behaviors and screens for NCDs opportunistically. It also works to establish NCD clinics and strengthen infrastructure for NCD care.













































































