Downloaded 117 times
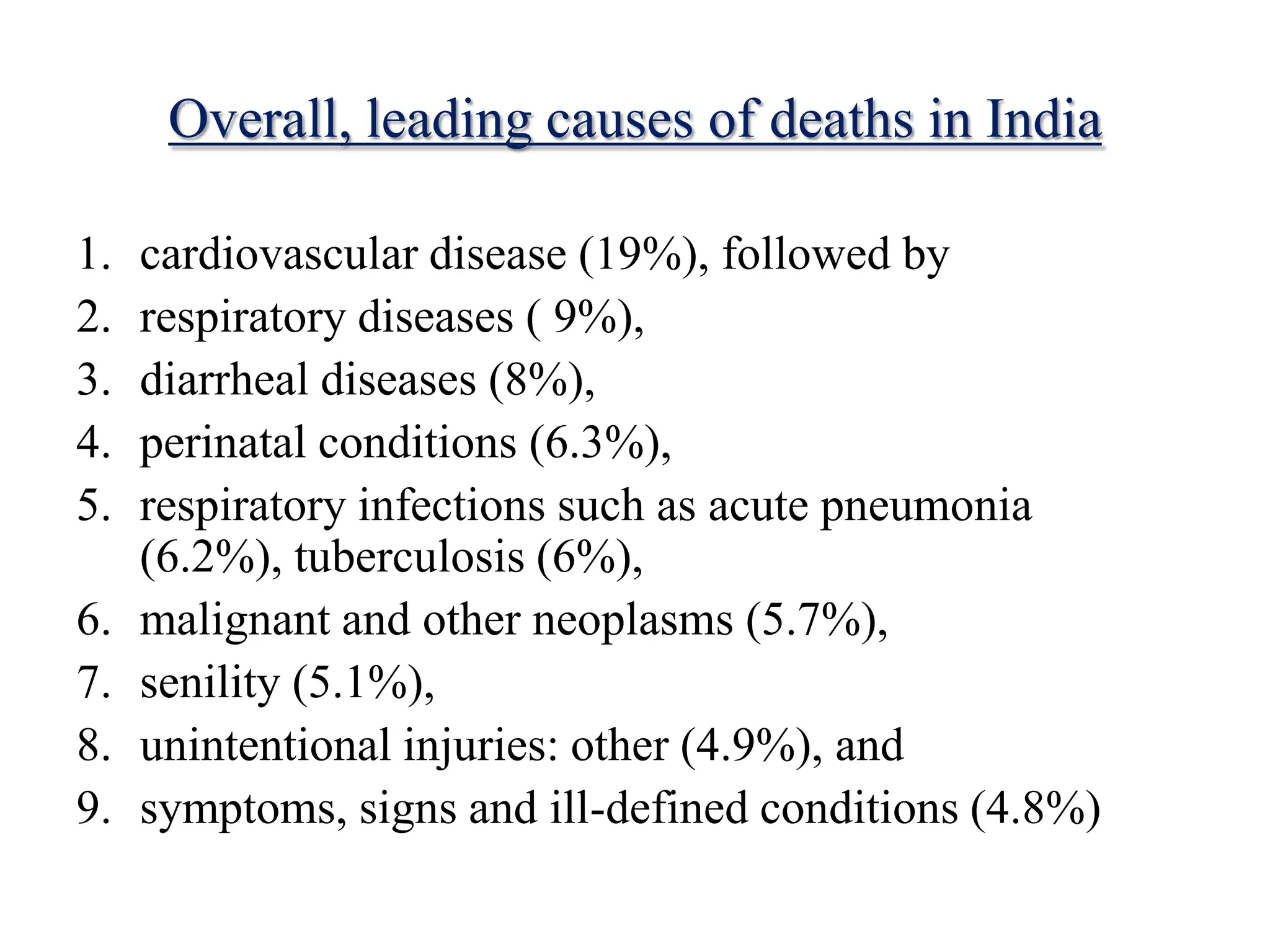
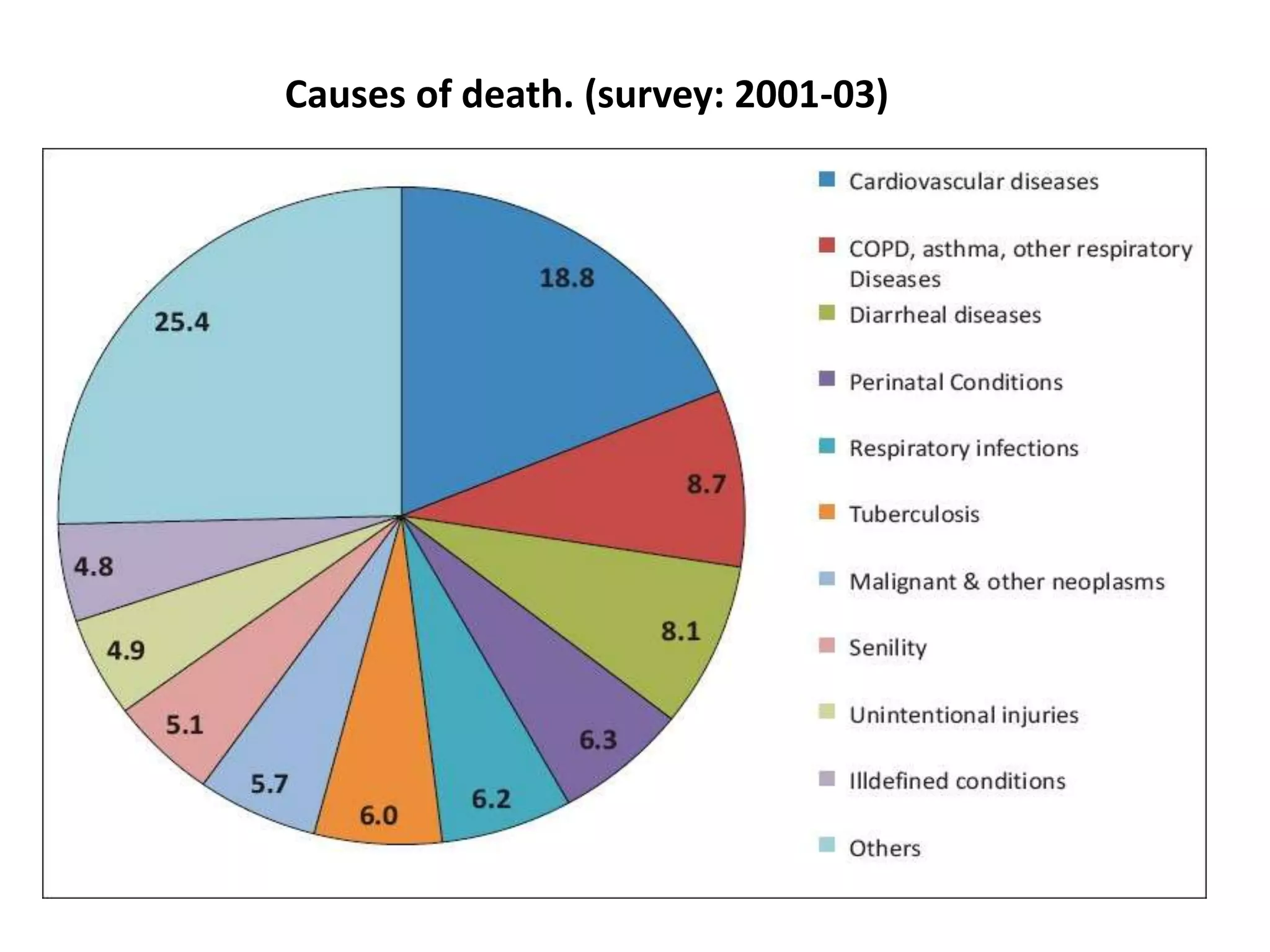
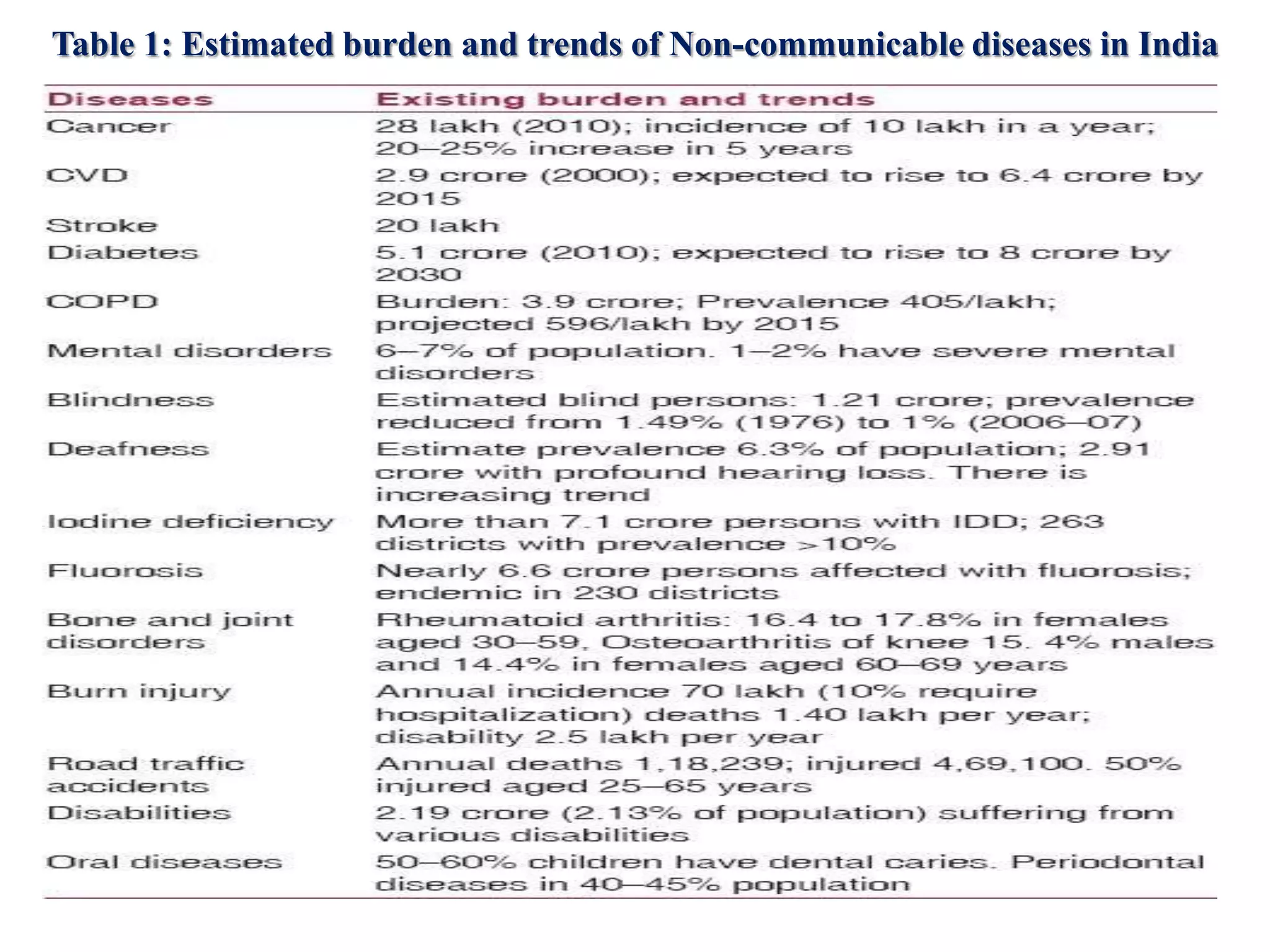
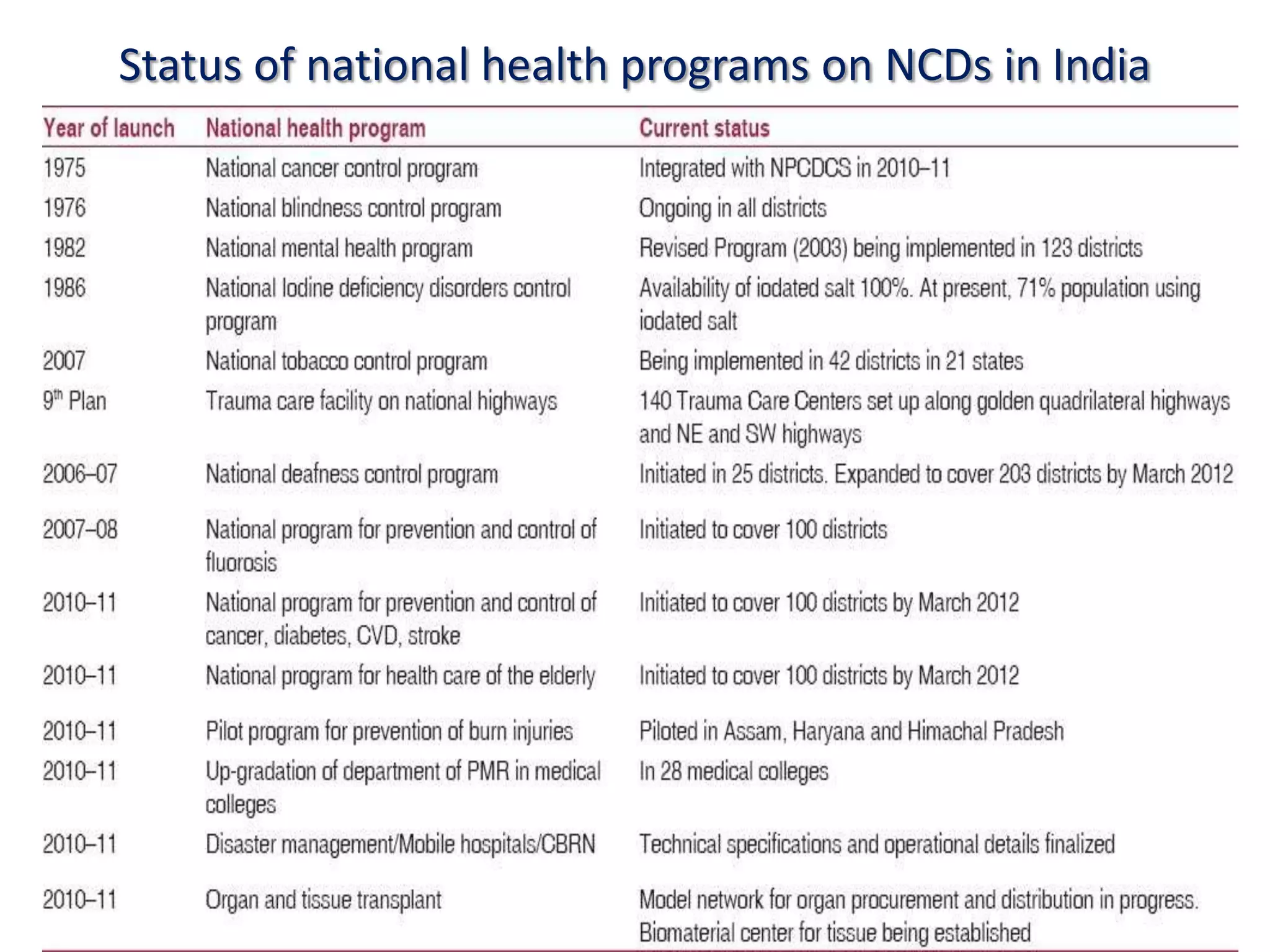


Chronic non-communicable diseases (NCDs) such as cardiovascular disease, cancer, and diabetes now account for over half of deaths in India and place a large economic burden. The National Programme for Prevention and Control of Cancer, Diabetes, CVD and Strokes (NPCDCS) aims to address NCDs through health promotion, screening, diagnosis, management, and capacity building integrated into primary healthcare. Current programs have had limited implementation; a comprehensive and widespread approach is still needed to reduce the growing NCD burden in India.