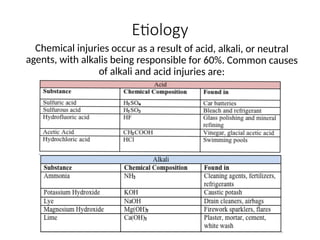
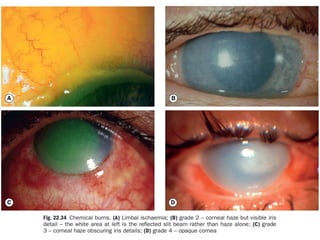
The document discusses non-mechanical ocular injuries, focusing on types such as chemical, thermal, and radiational injuries. It details the causes, pathophysiology, diagnosis, management, and treatment options for these injuries, emphasizing the importance of early irrigation for chemical burns. Additionally, the document outlines classification schemes for corneal burns and highlights follow-up care and potential long-term complications.





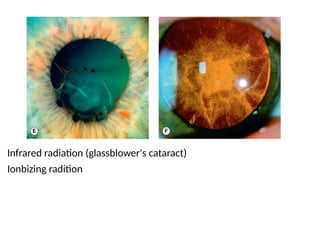























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











