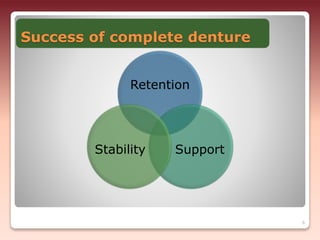
This document discusses factors that influence the stability of complete dentures. It defines stability as the quality of a removable prosthesis to resist displacement from functional stresses. The three main factors discussed are:
1) The relationship of the denture base to underlying tissues - Proper adaptation of the denture base to the residual ridges and surrounding tissues improves stability.
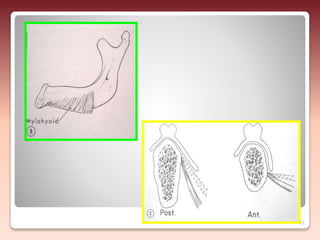
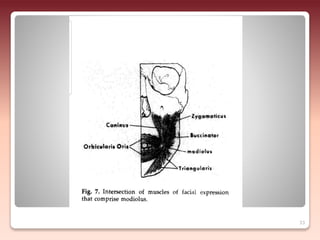
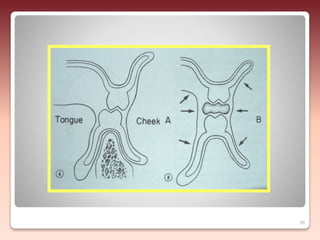
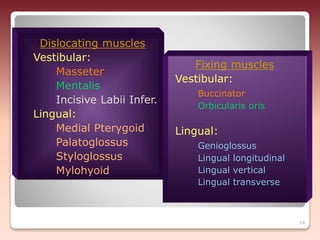
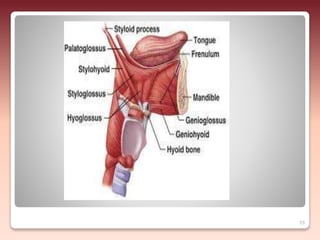
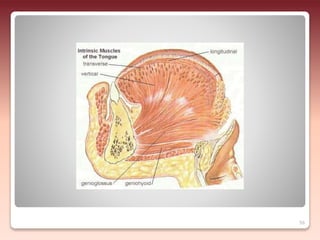
2) The relationship of the denture borders to surrounding muscles - Contouring the denture to allow free function of muscles like the buccinator and allowing muscles to help seat the denture enhances stability.
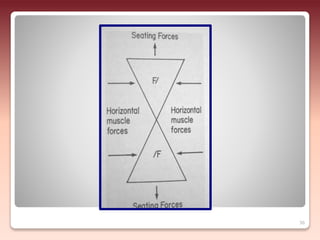
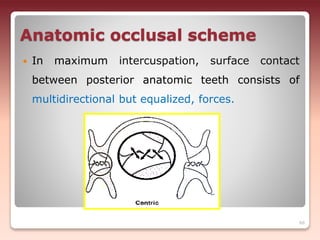
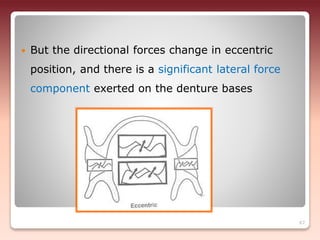
3) The relationship of opposing occlusal surfaces - Proper occlusal harmony contributes to resisting forces that could displace the dentures.


































![Stability in Complete Denture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stabilityincompletedentureautosaved-260115125839-4ff5a430-thumbnail.jpg?width=640&height=640&fit=bounds)












































