Downloaded 12 times
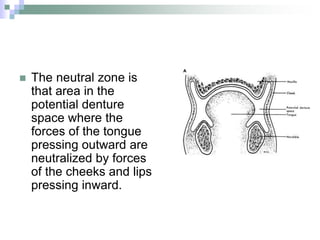




The document discusses the neutral zone concept in complete dentures, emphasizing the importance of harmonizing dentures with normal neuromuscular function to ensure stability and comfort for edentulous patients. It covers definitions, anatomical aspects, literature reviews, and various techniques for recording and fabricating dentures based on the neutral zone principle, which is the area where opposing muscle forces are balanced. The findings indicate that proper denture design and techniques can significantly enhance patient satisfaction and denture performance.



































































