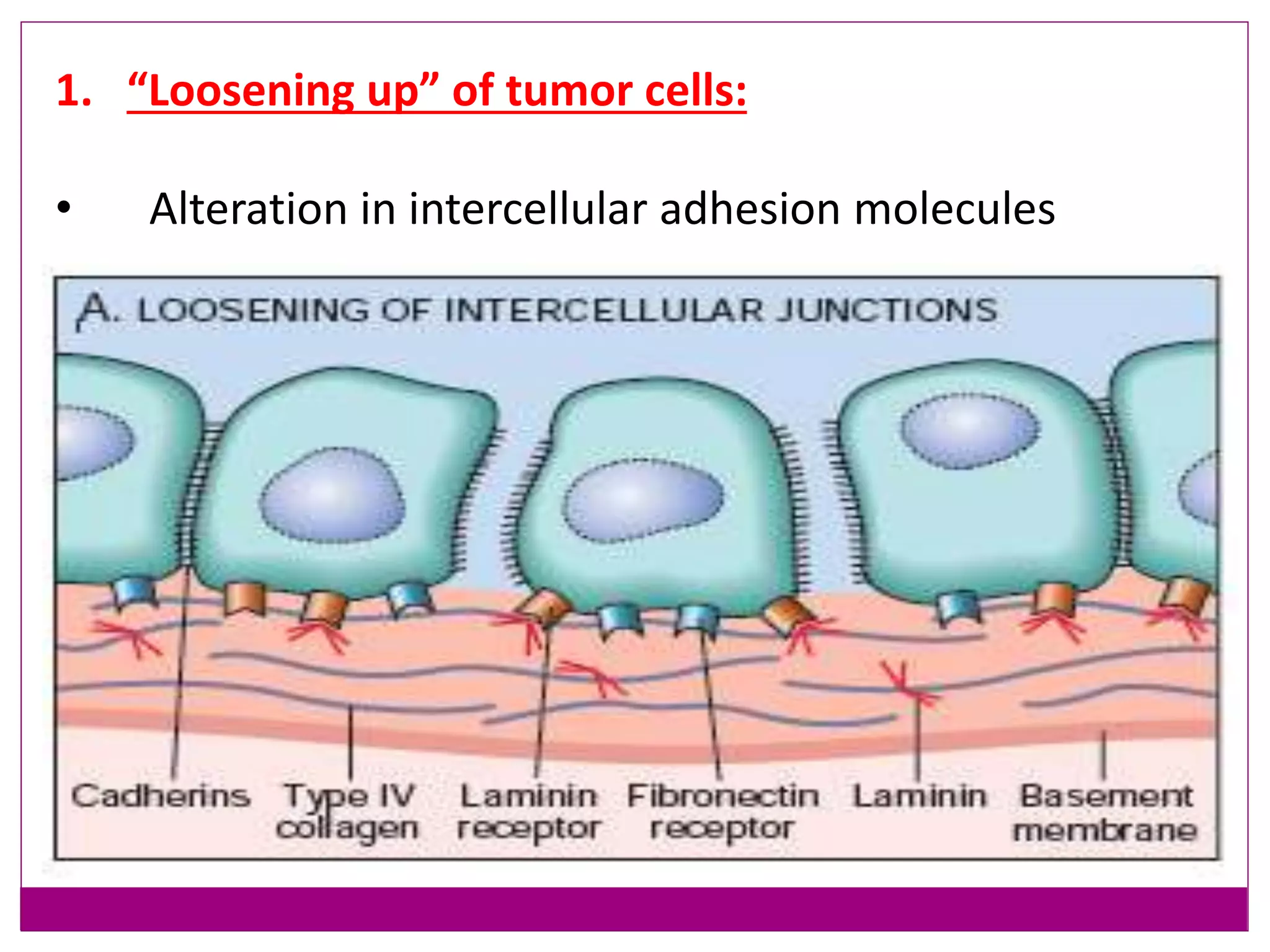
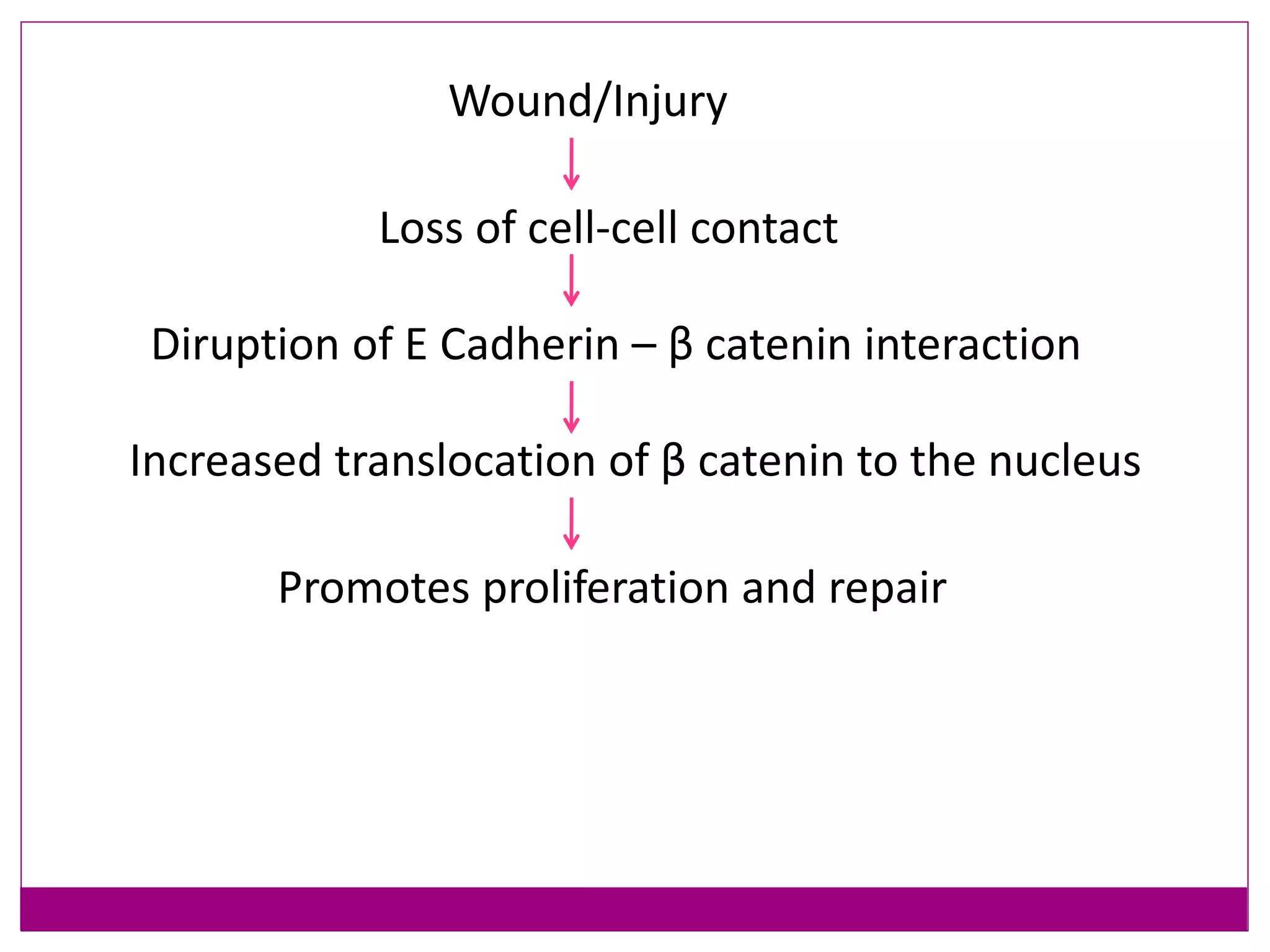
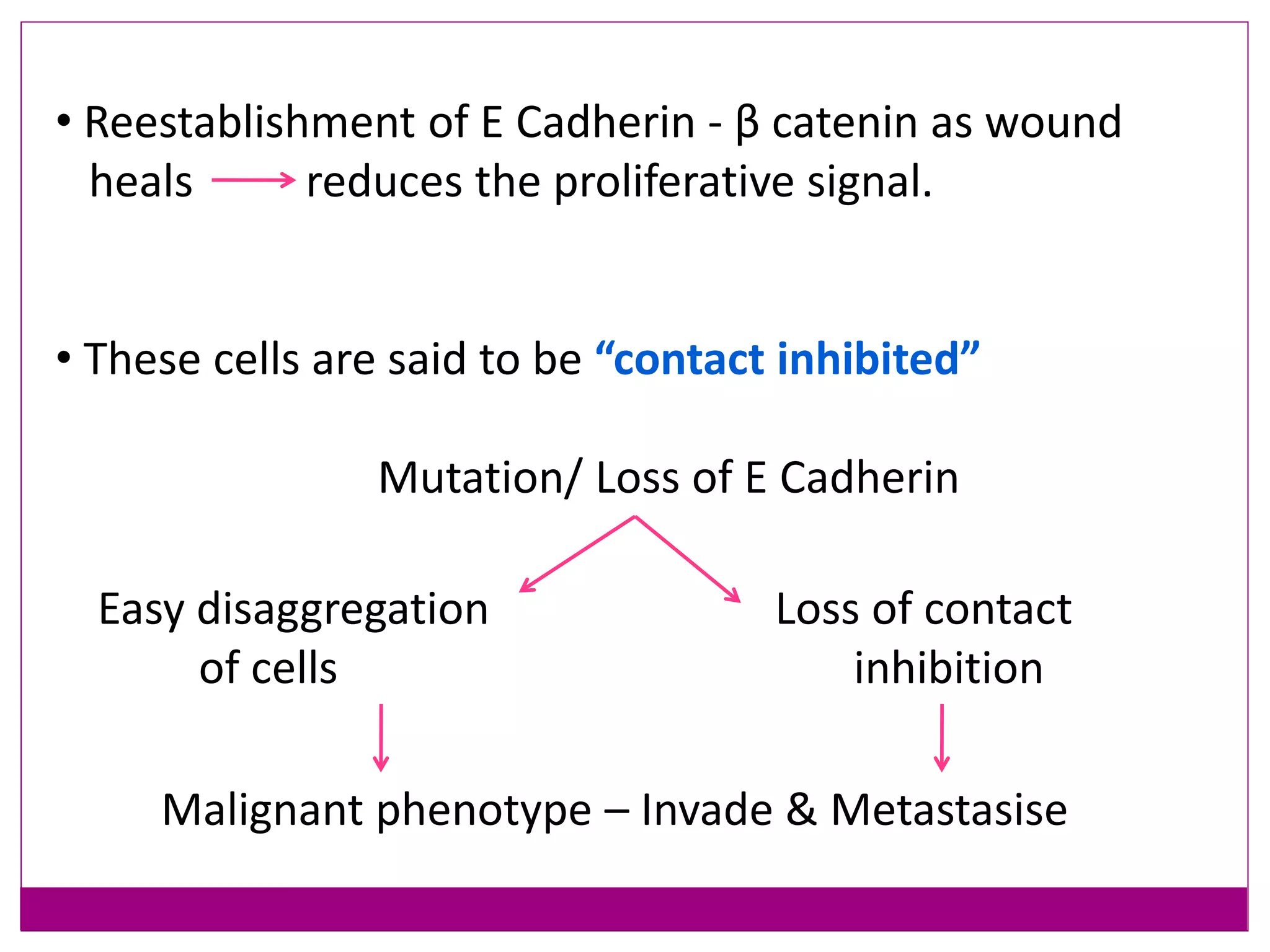
This document provides an overview of cancer metastasis and the epithelial-mesenchymal transition (EMT) process. It discusses the metastatic cascade, which involves tumor cell invasion, intravasation into blood vessels, transport through circulation, extravasation and homing to distant sites, and formation of secondary tumors. EMT is described as a key step in metastasis that allows epithelial cells to detach from primary tumors and migrate. The molecular and cellular changes involved in EMT include loss of epithelial markers like E-cadherin and gain of mesenchymal markers. Transcription factors such as Snail, Slug, Twist, and ZEB play important roles in inducing EMT. Understanding metastasis and EMT can help develop strategies to prevent cancer spread