Downloaded 22 times

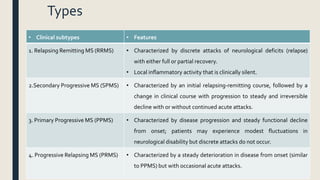
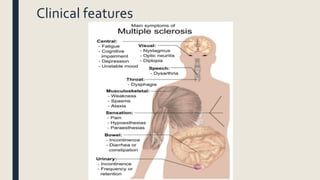
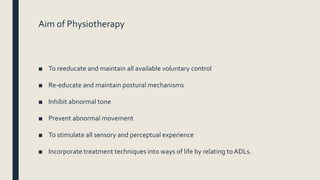
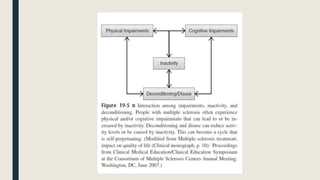
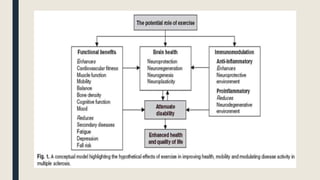
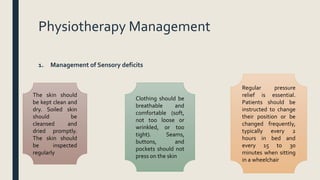
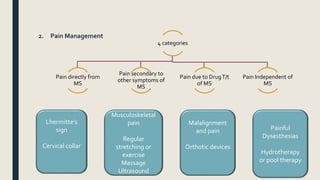

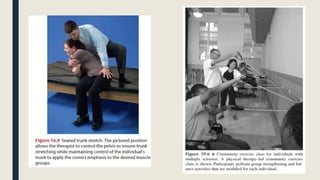








The document discusses physiotherapy for managing multiple sclerosis (MS), detailing its clinical features, physiotherapy roles, and management strategies for various symptoms such as sensory deficits, pain, fatigue, spasticity, balance, and swallowing. It also highlights recent advances in physiotherapy interventions and their effectiveness, particularly regarding spasticity and pain management. The document concludes with references to key literature supporting these approaches.











































































