Downloaded 643 times
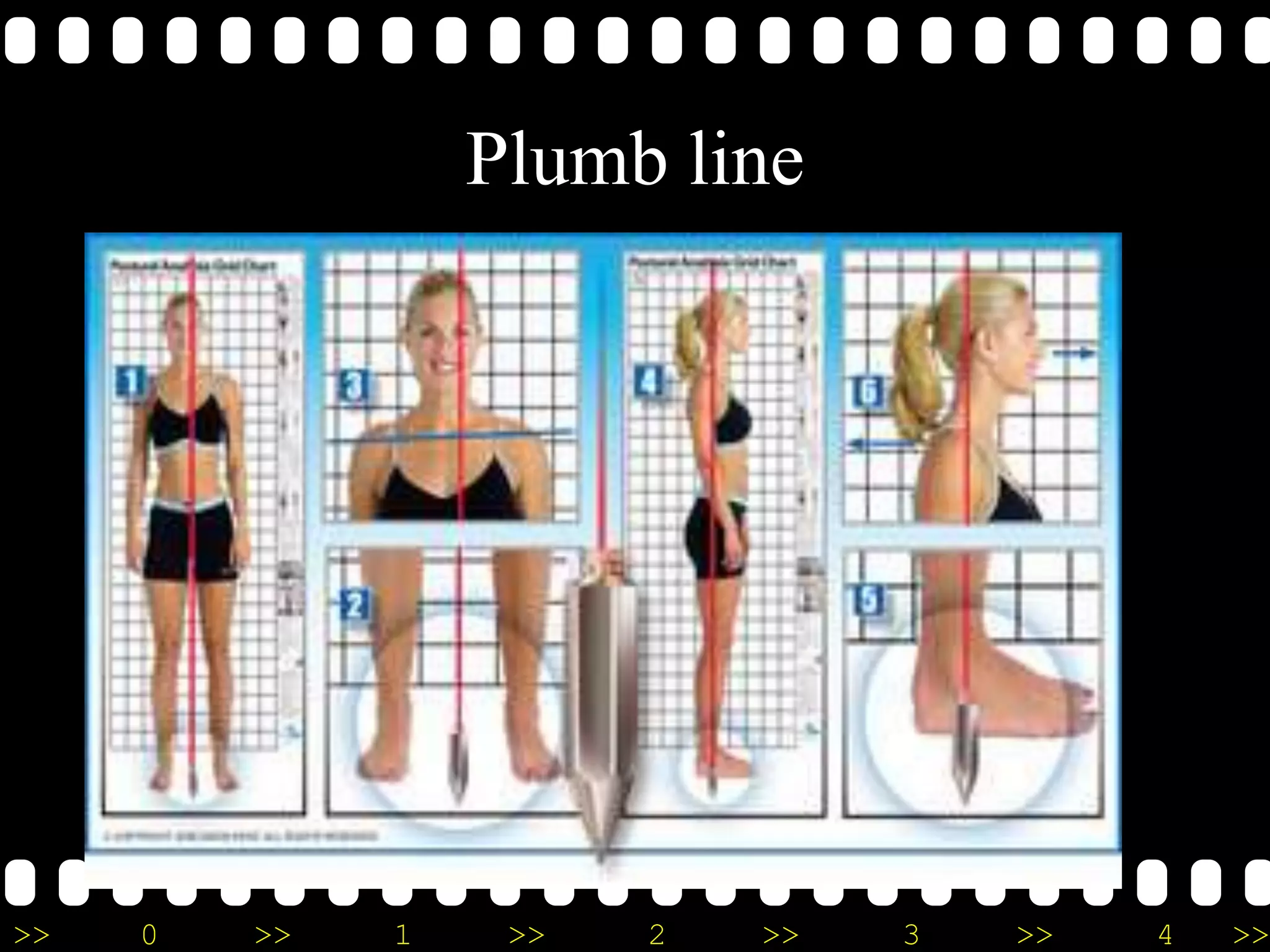
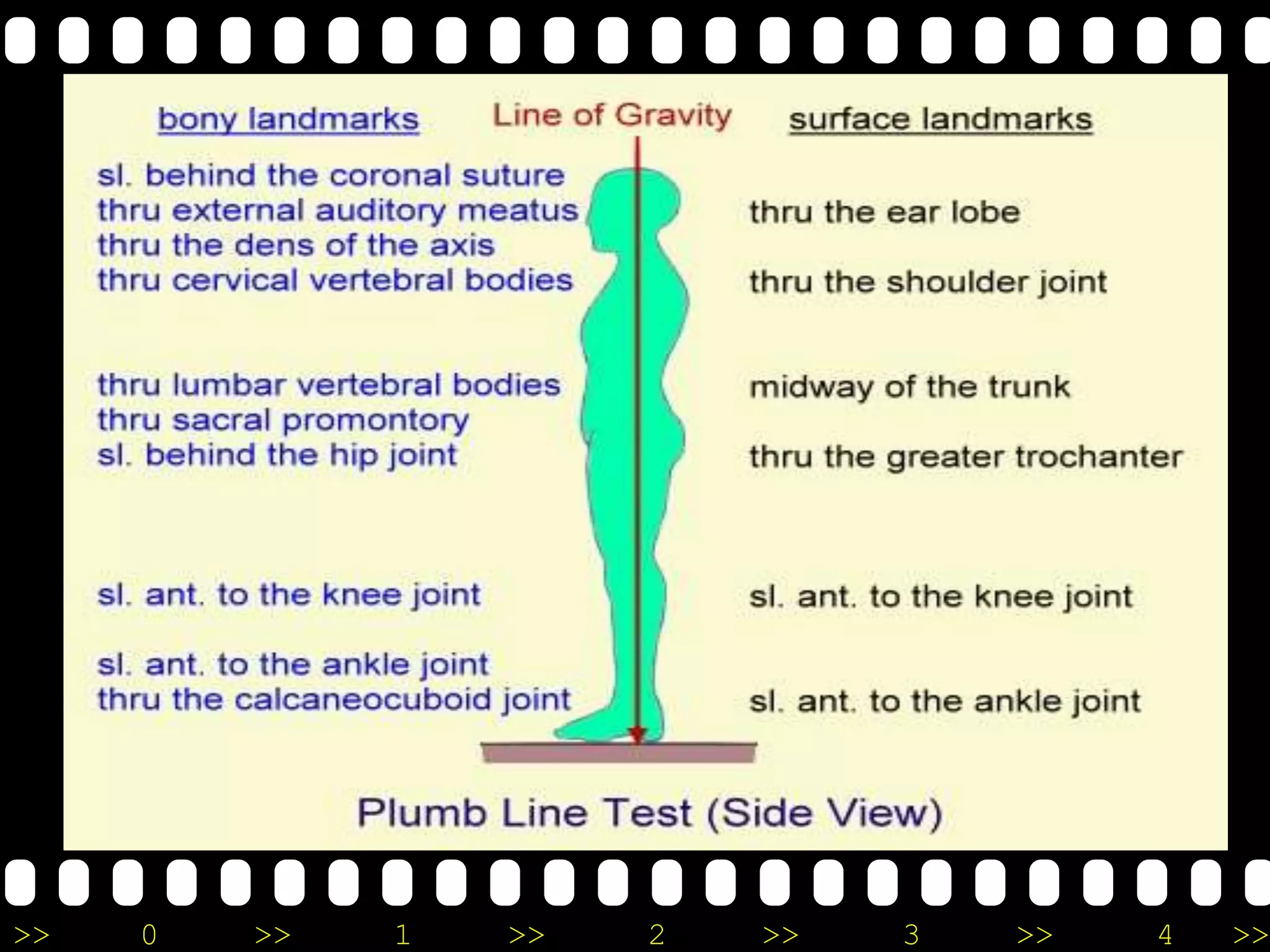
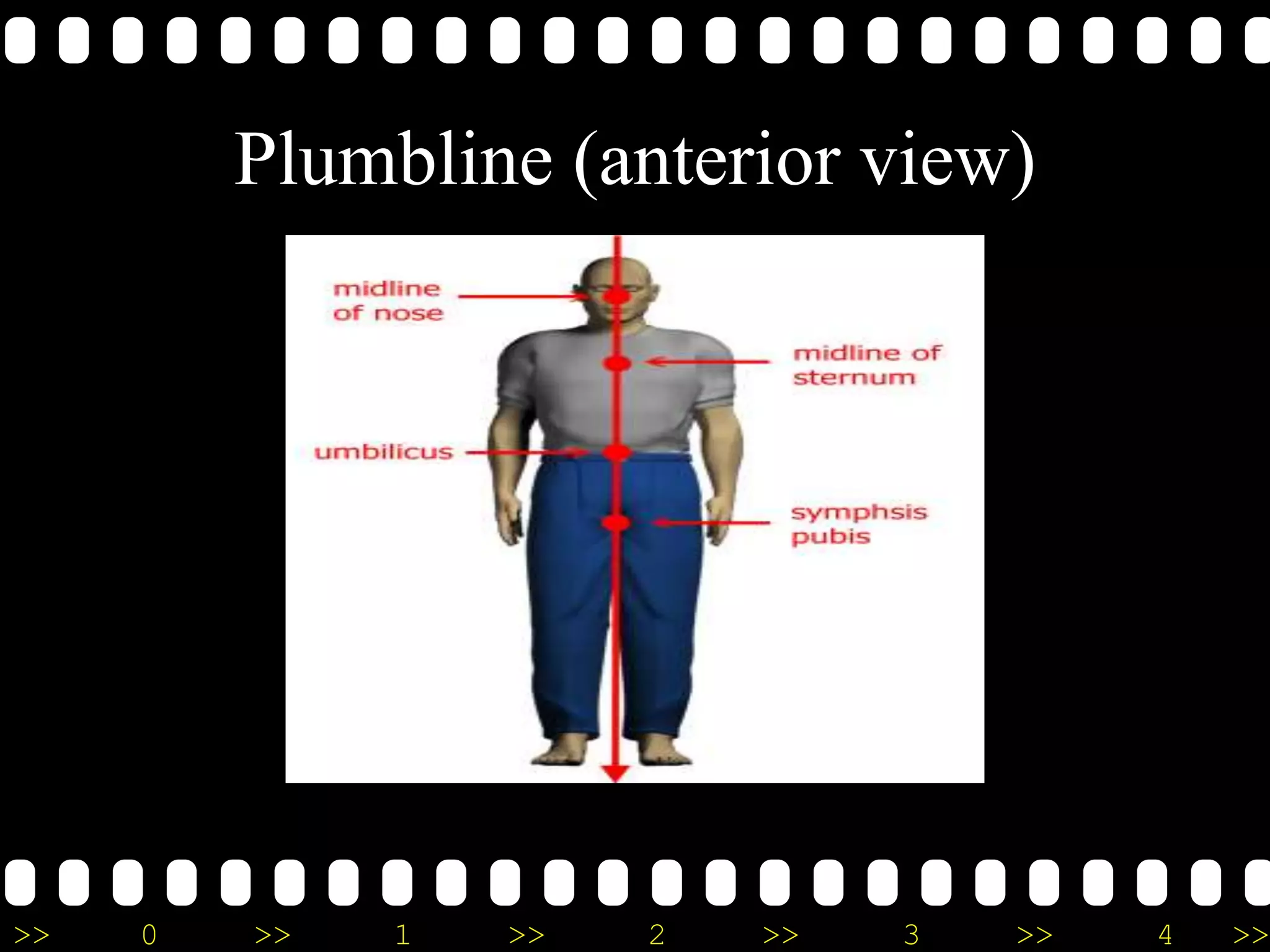
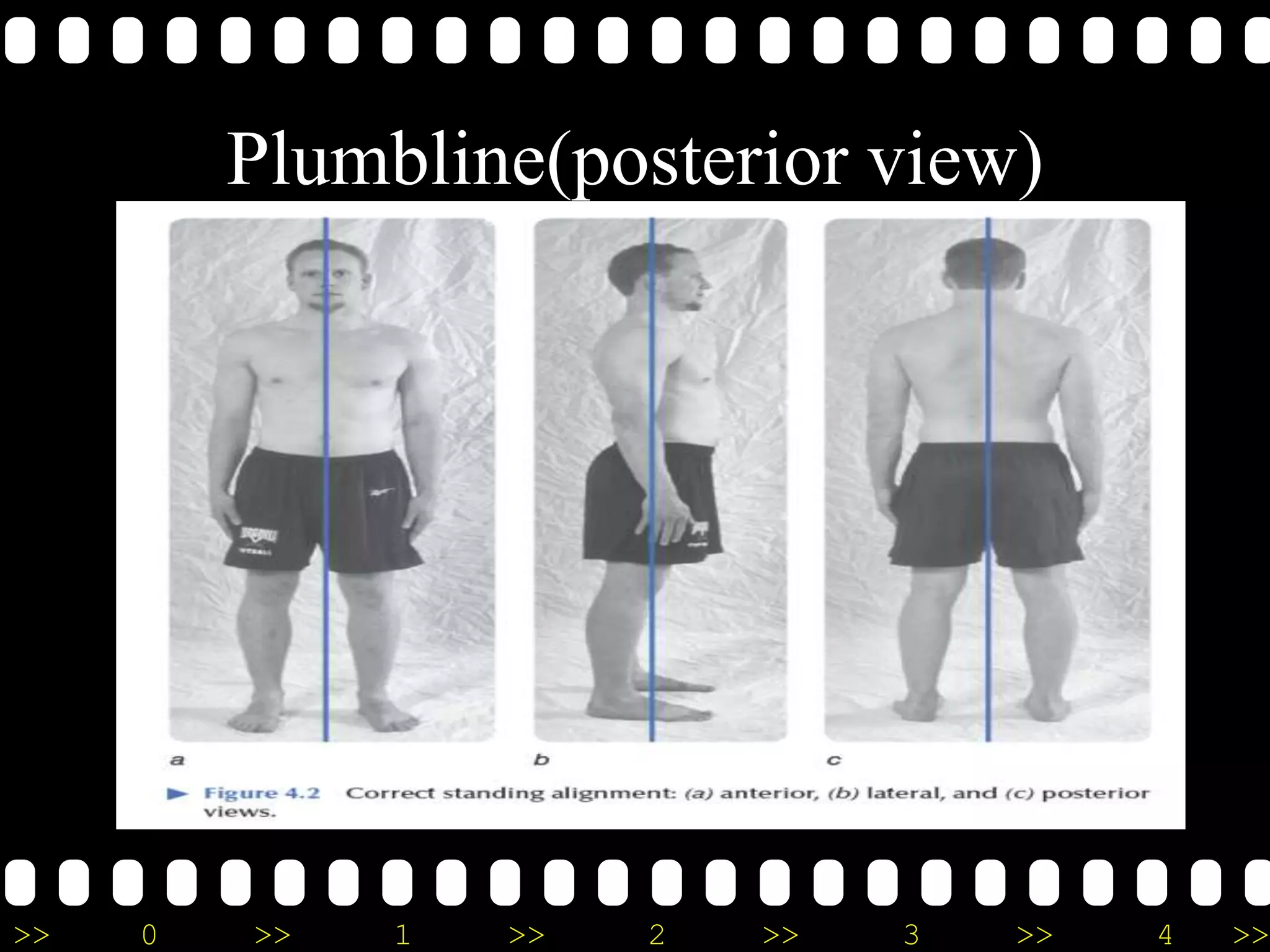
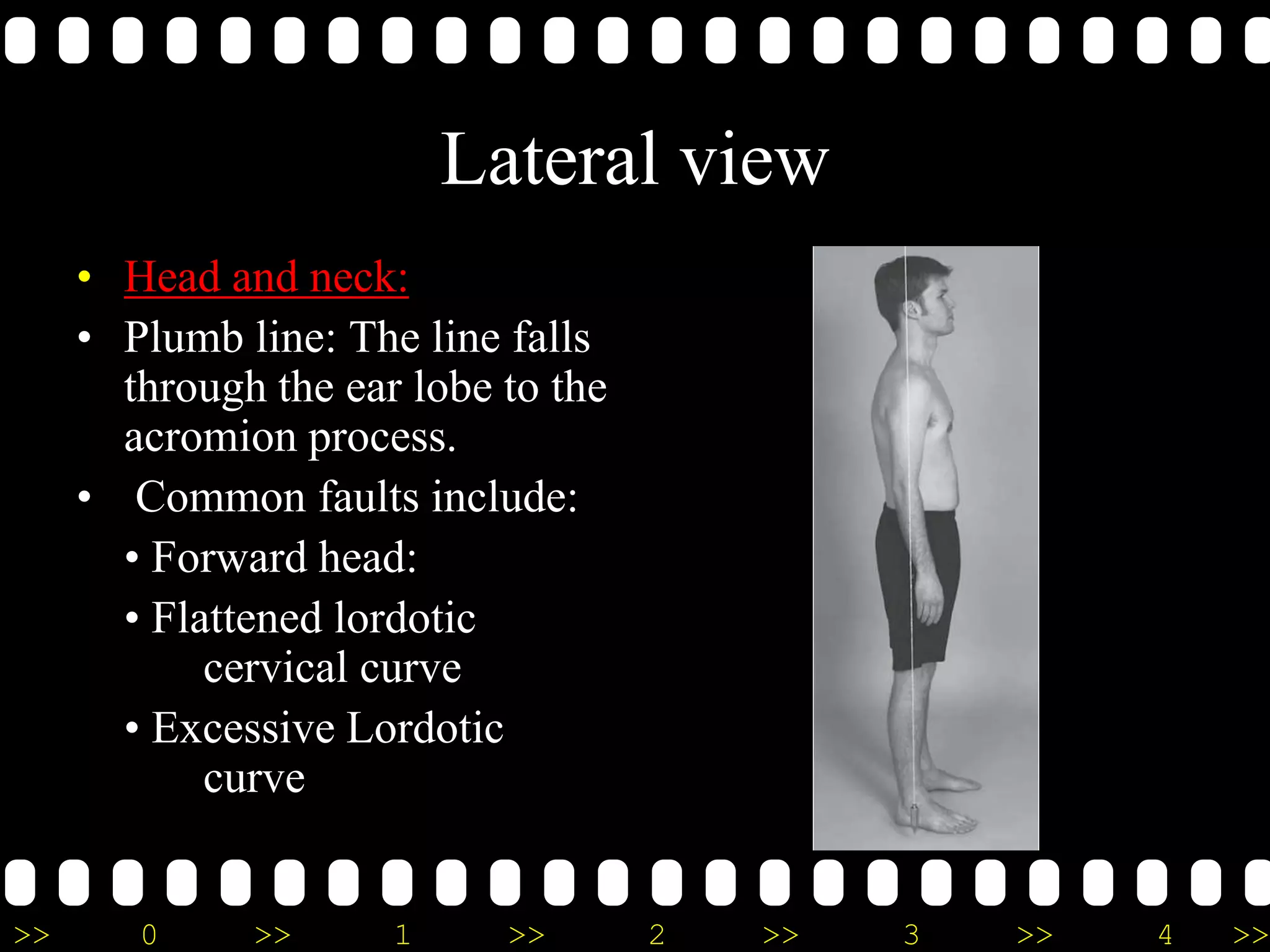
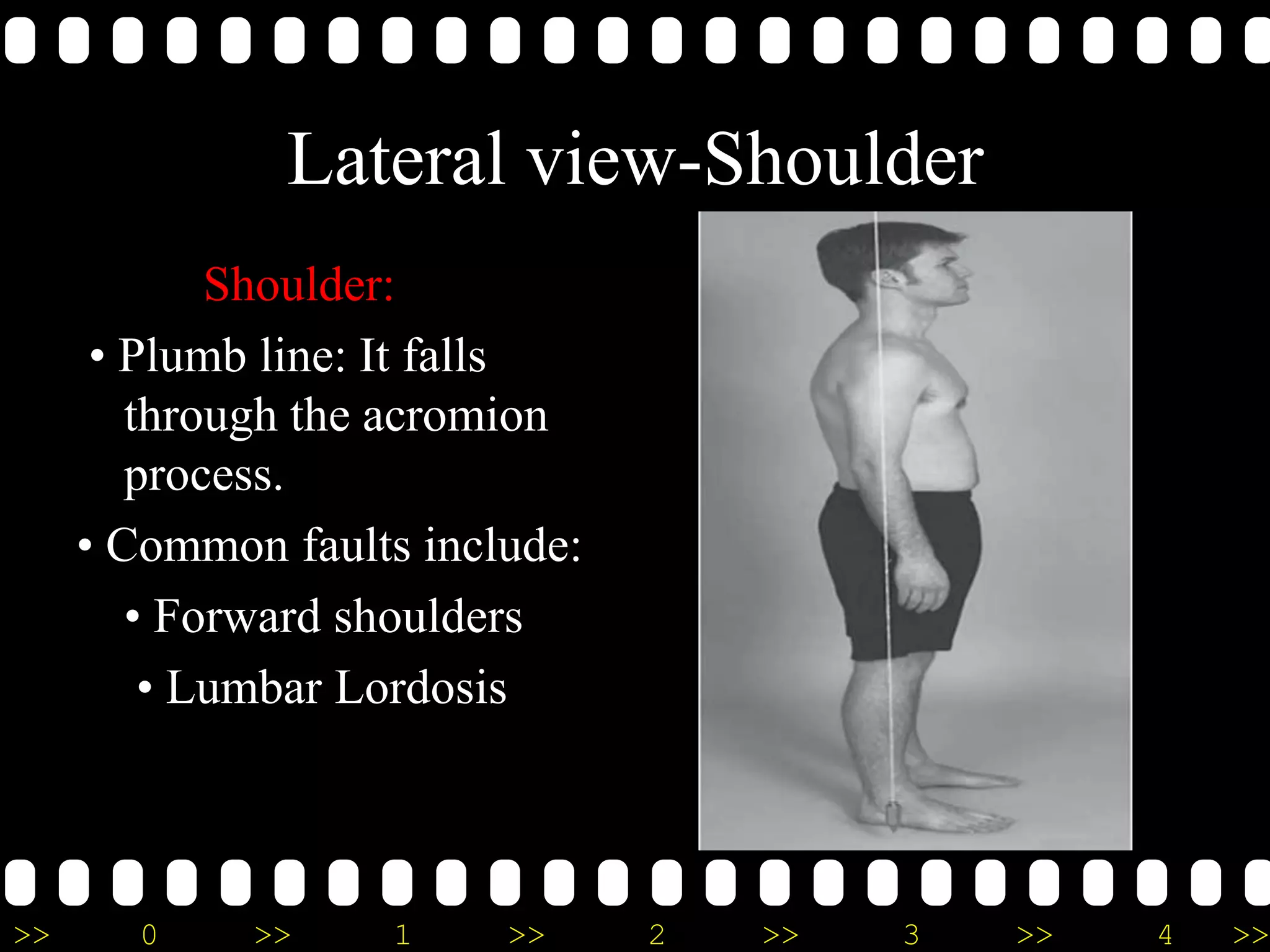
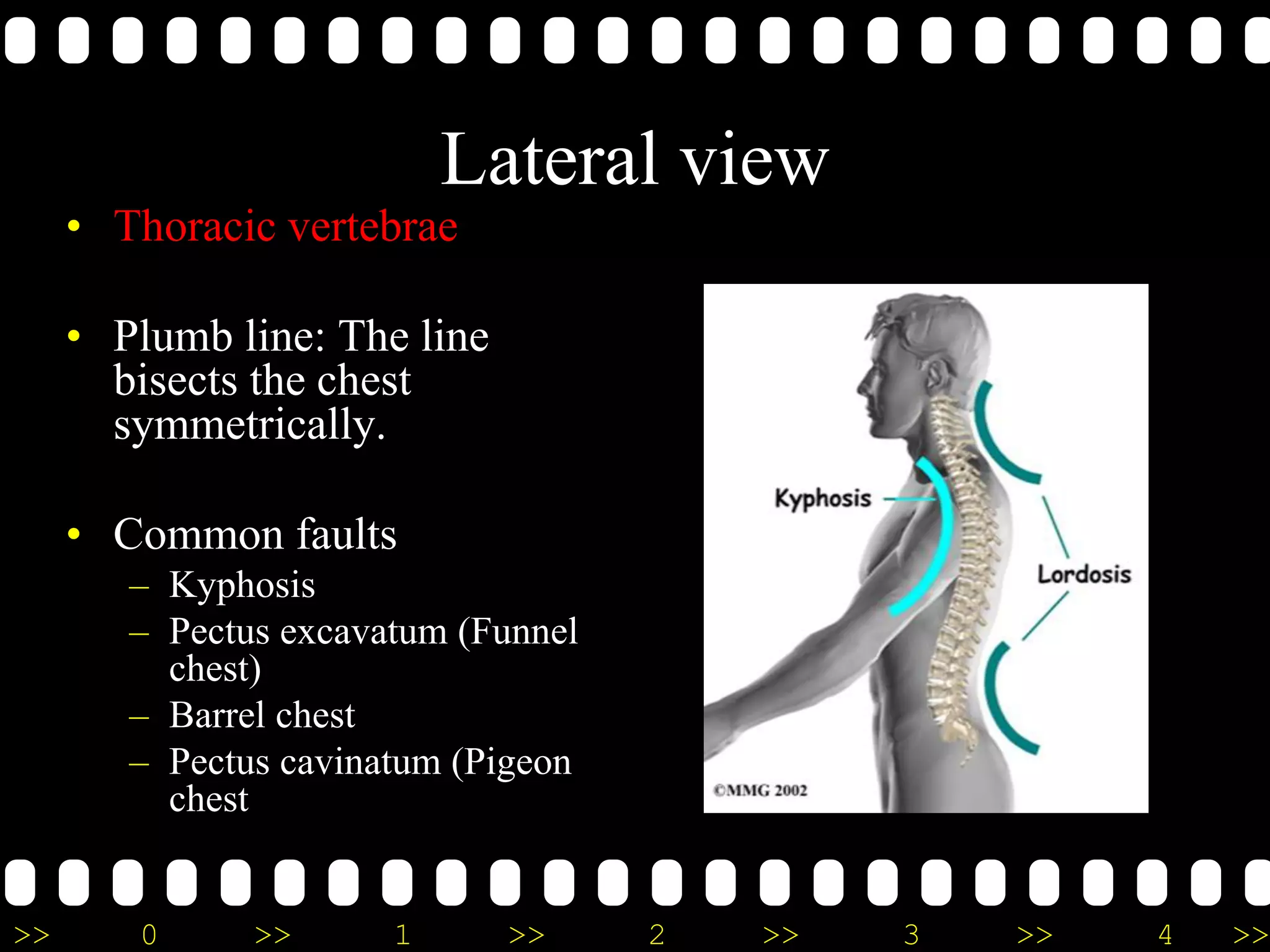
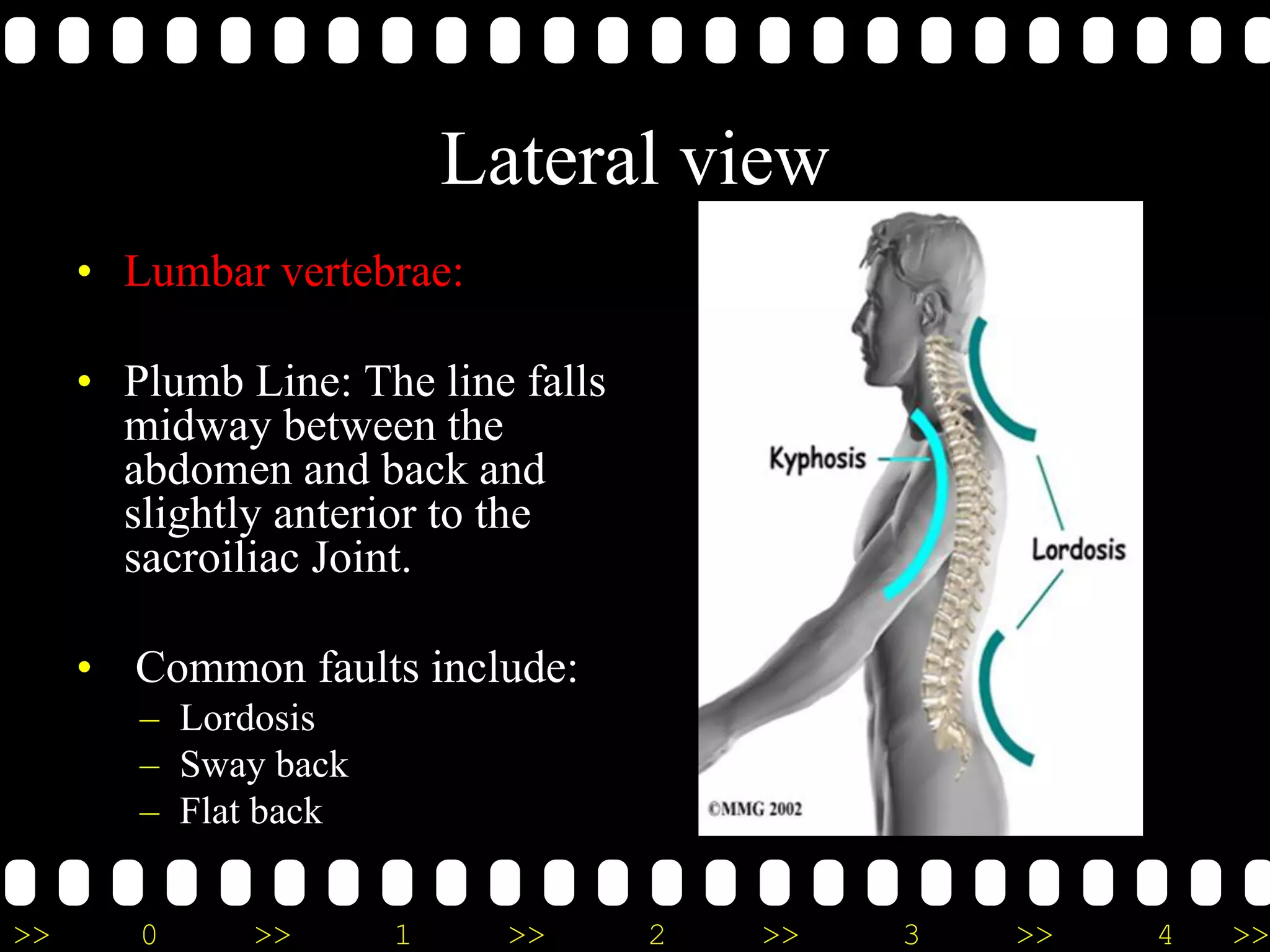
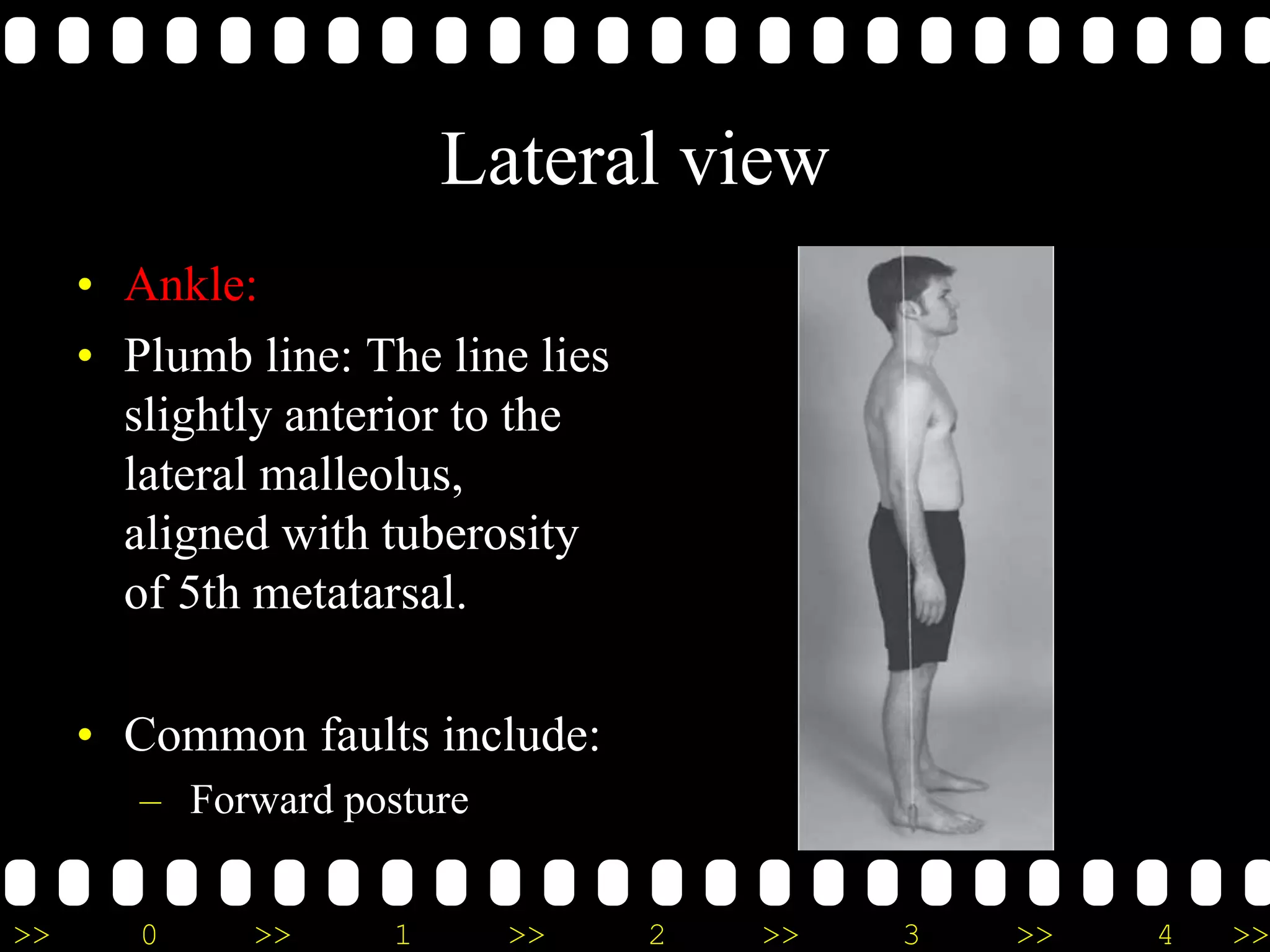
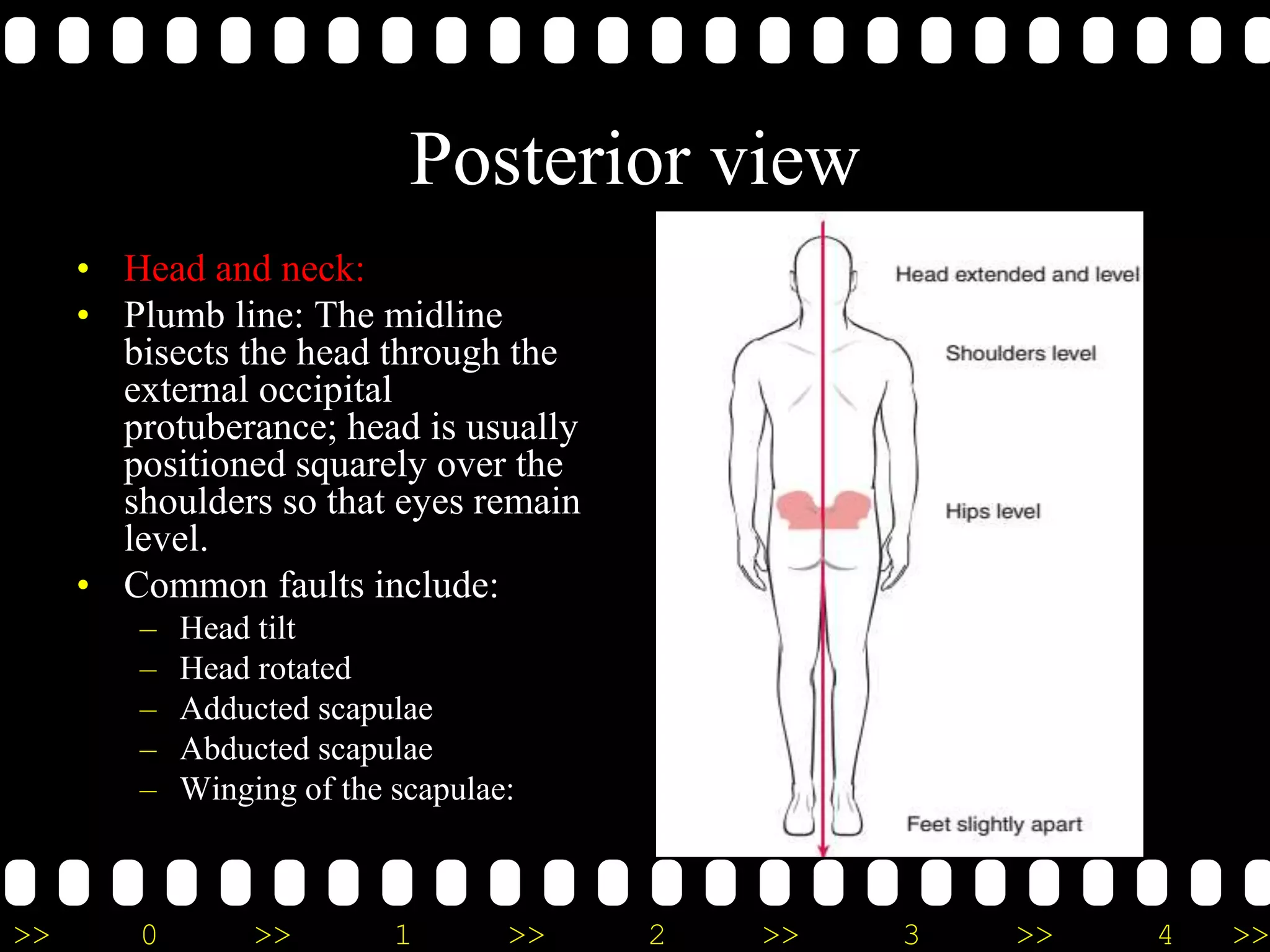
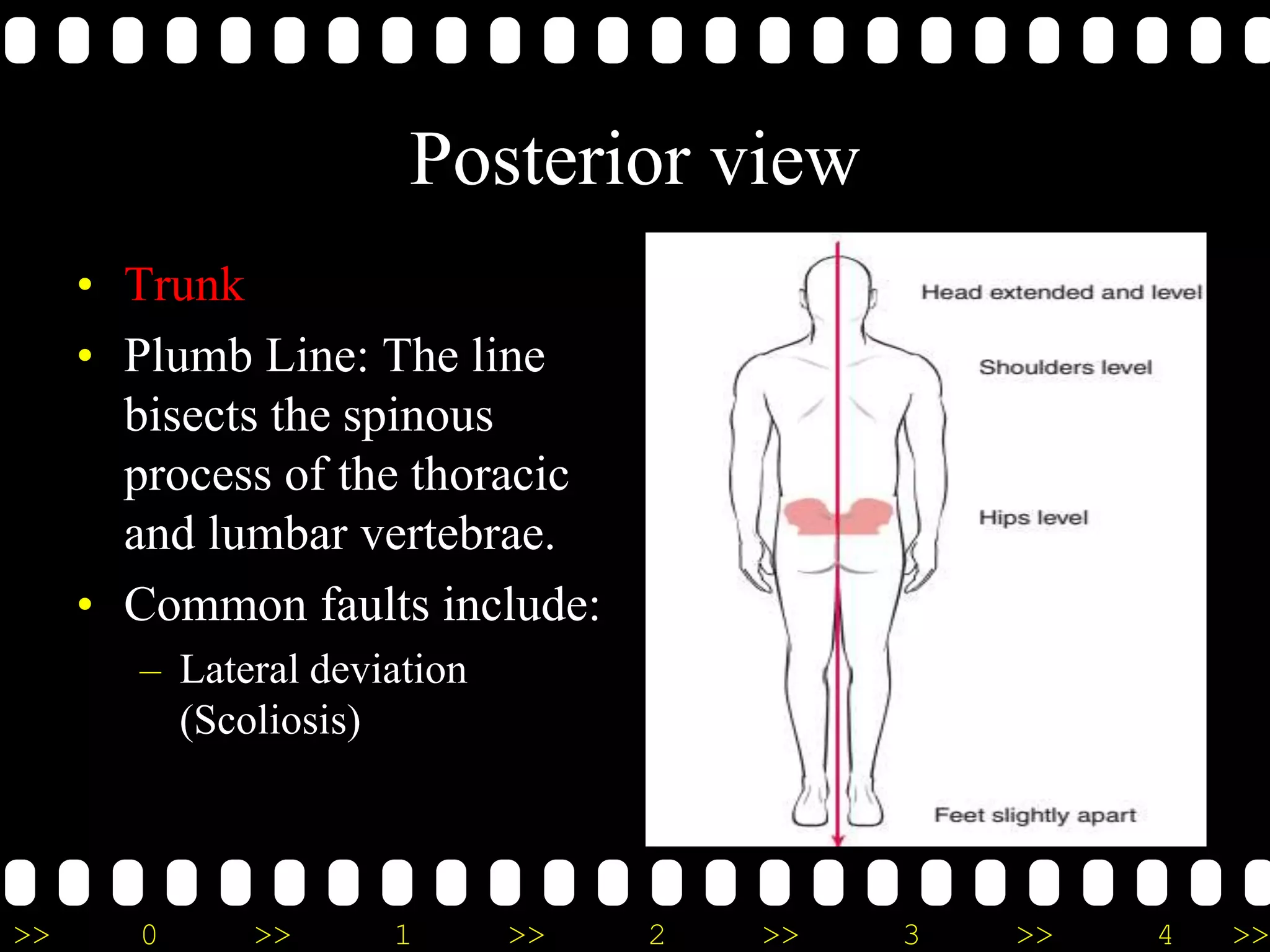
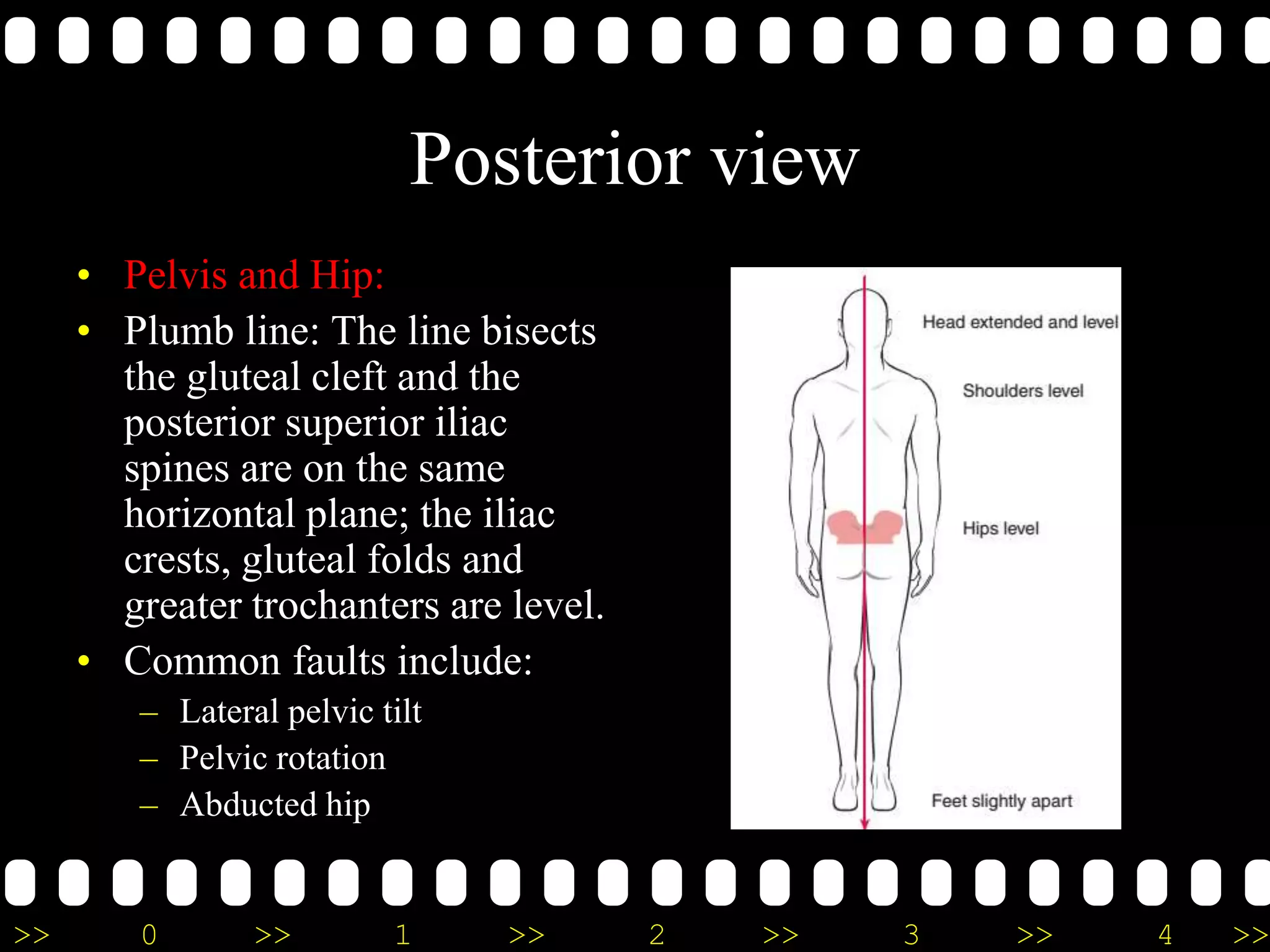
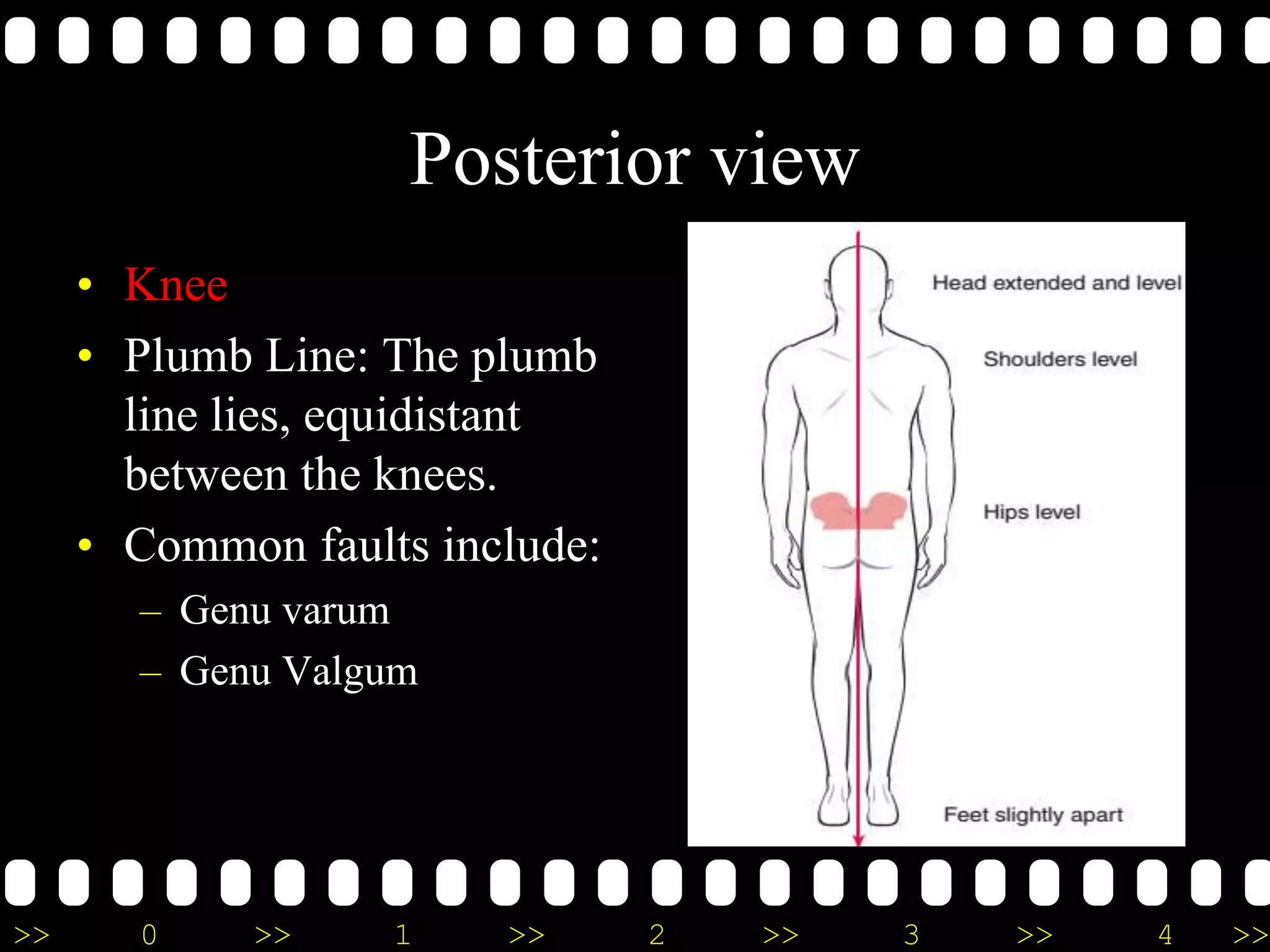
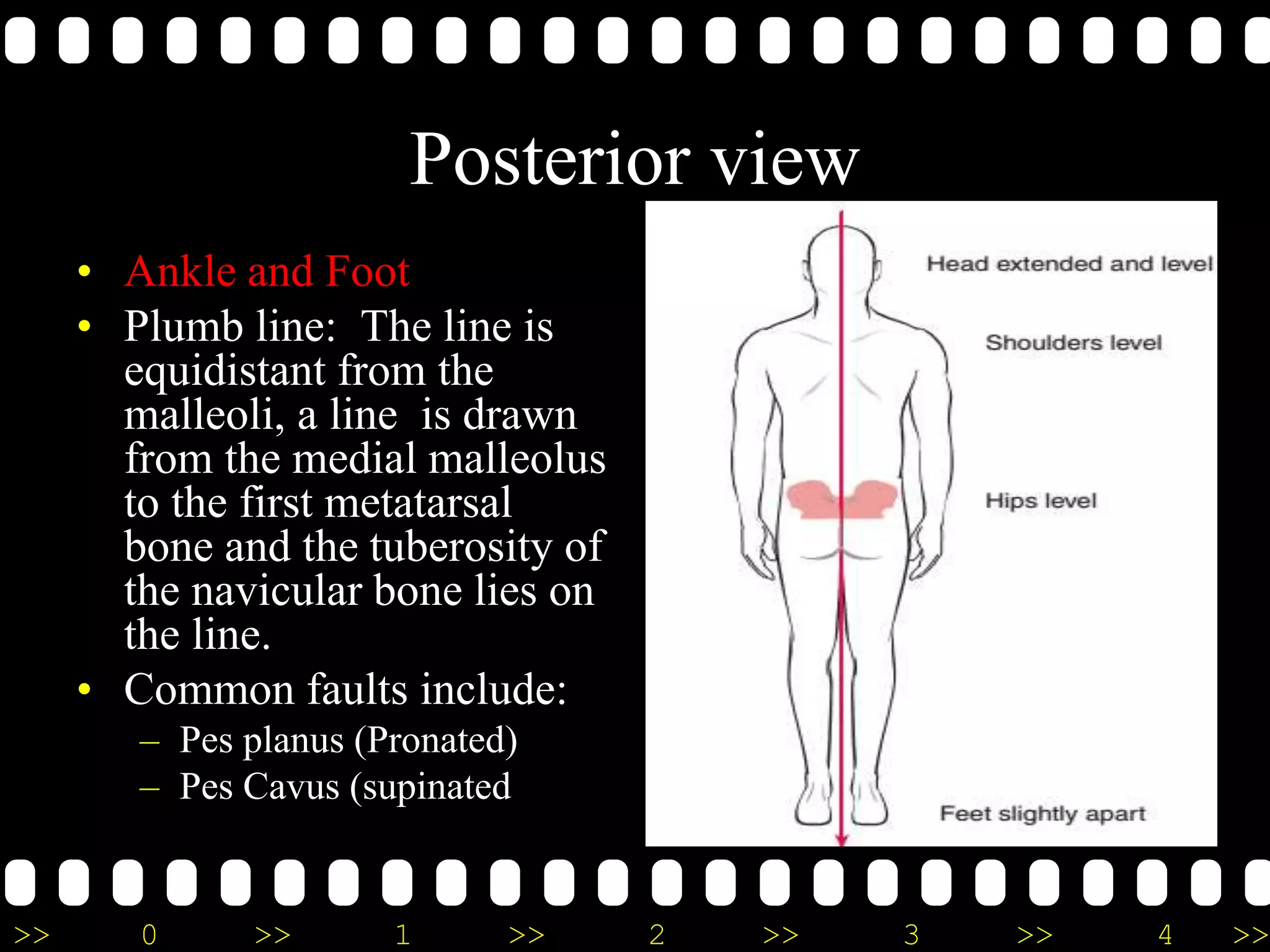
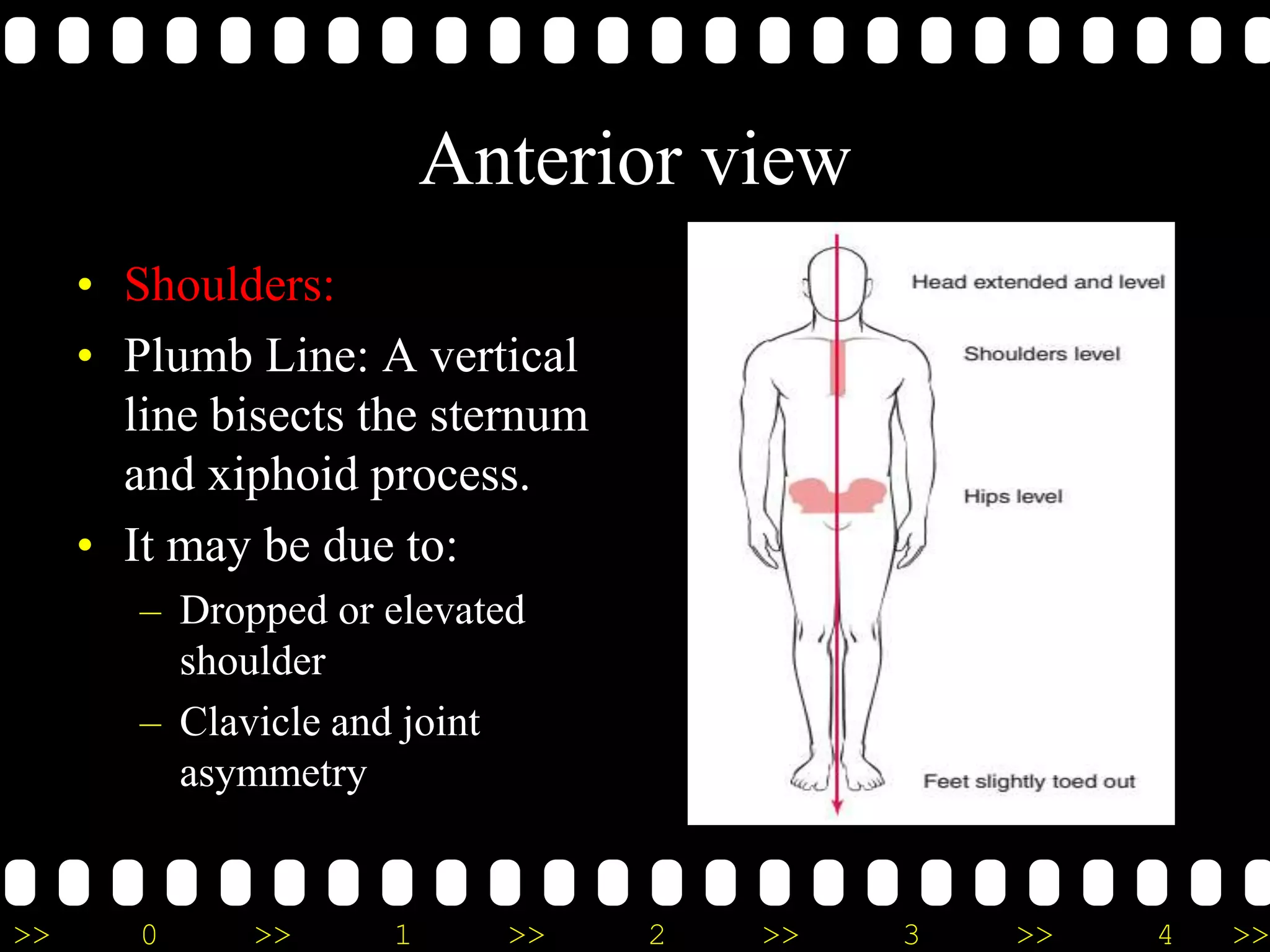
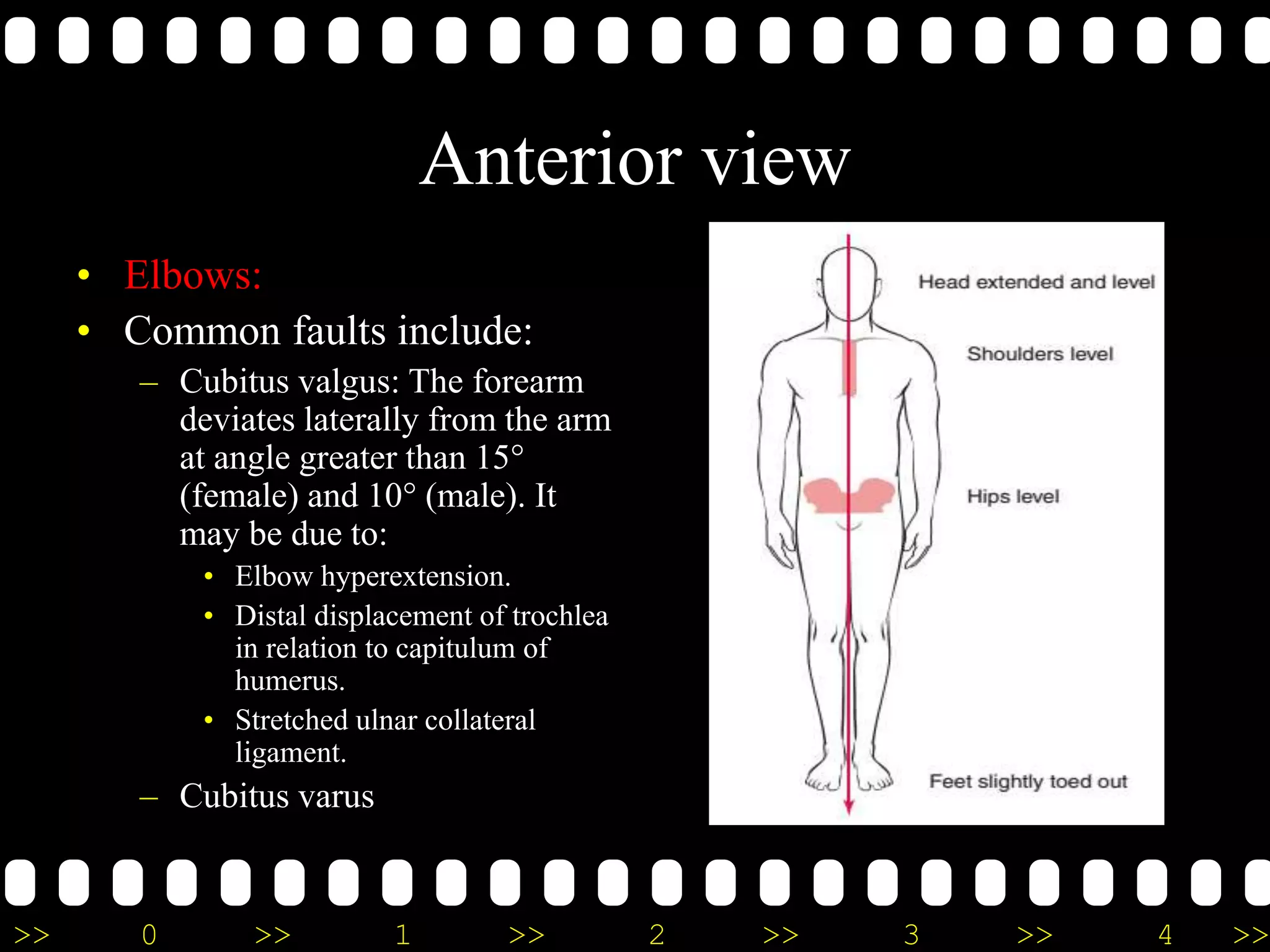
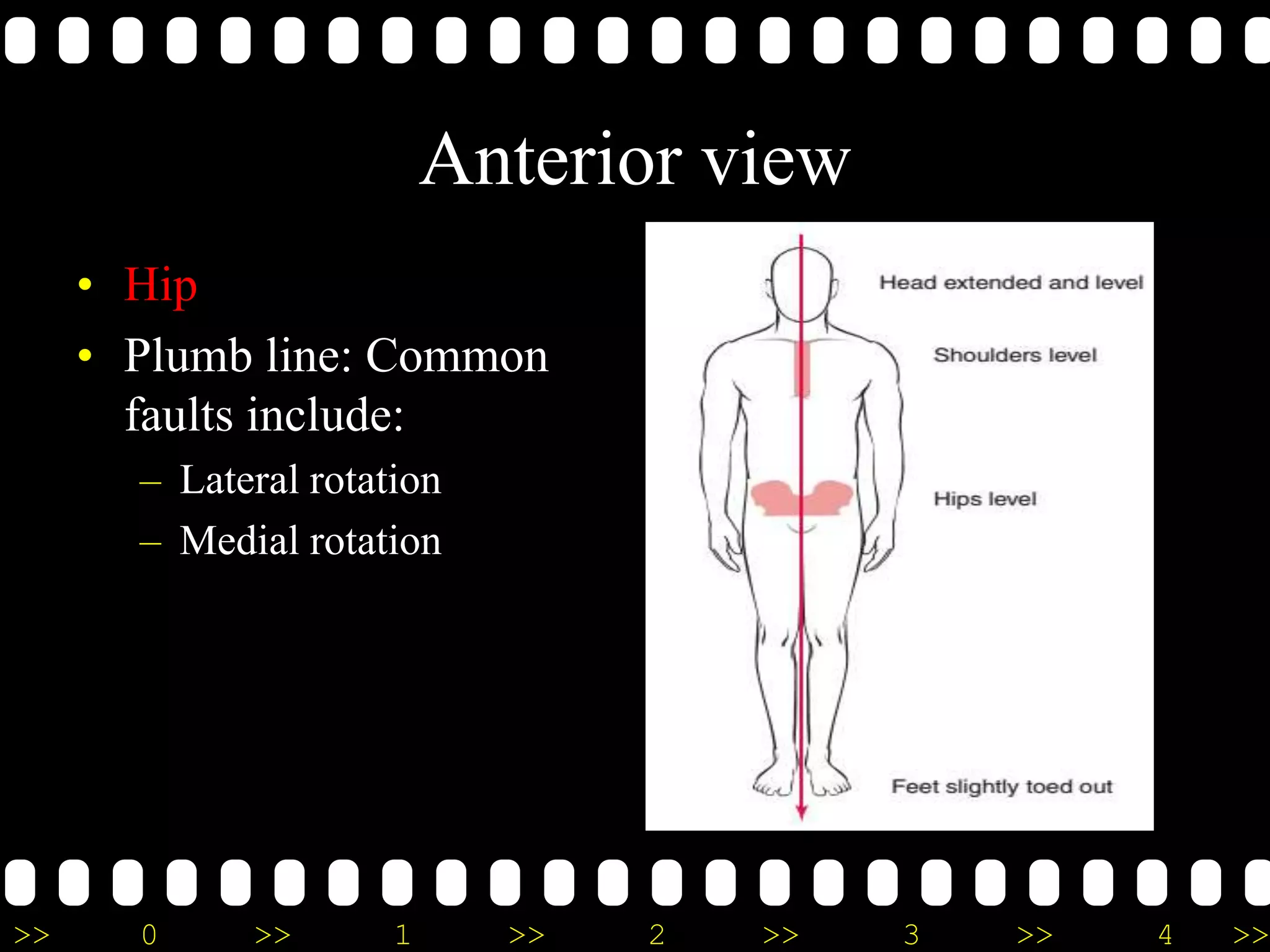
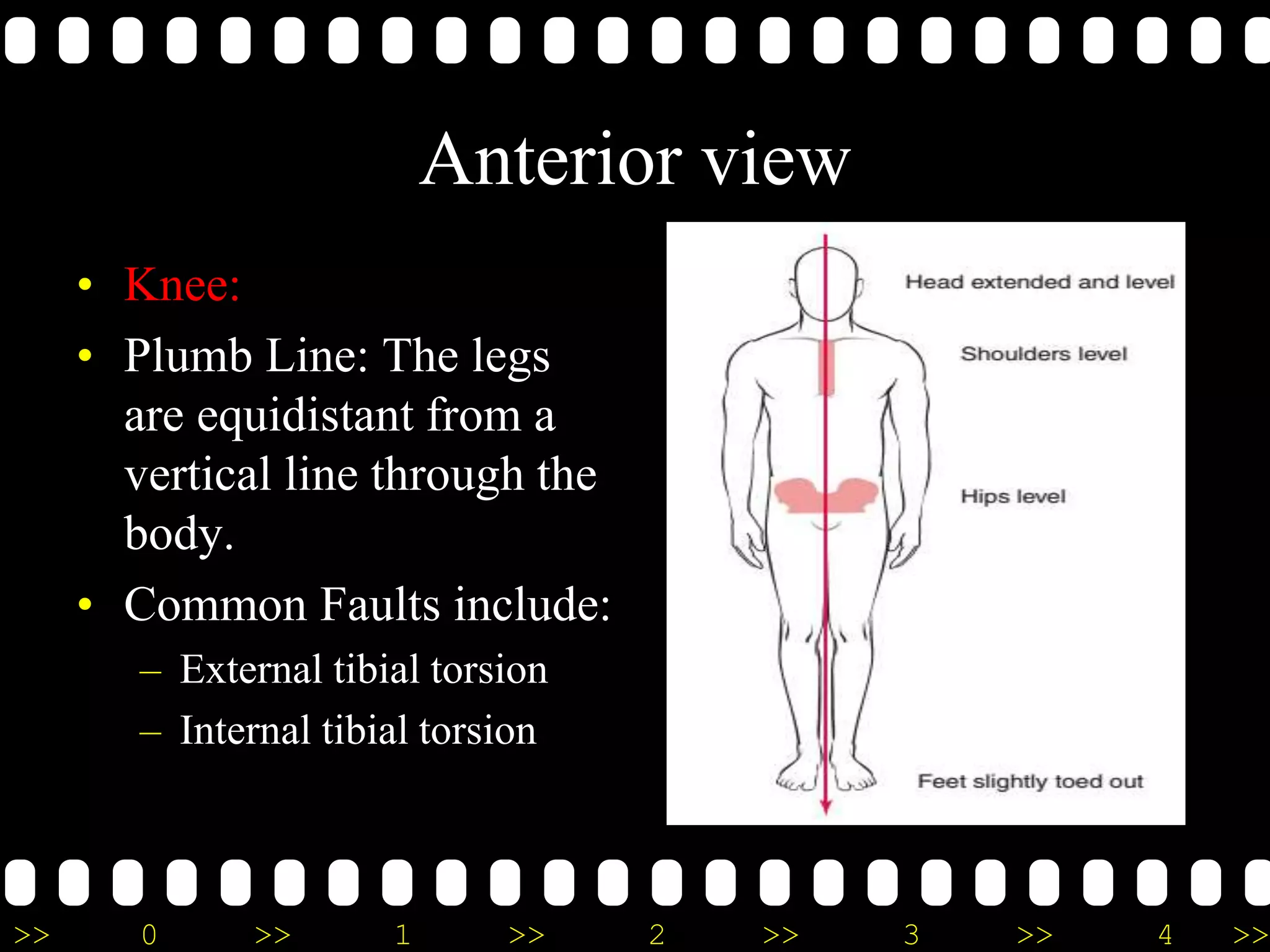
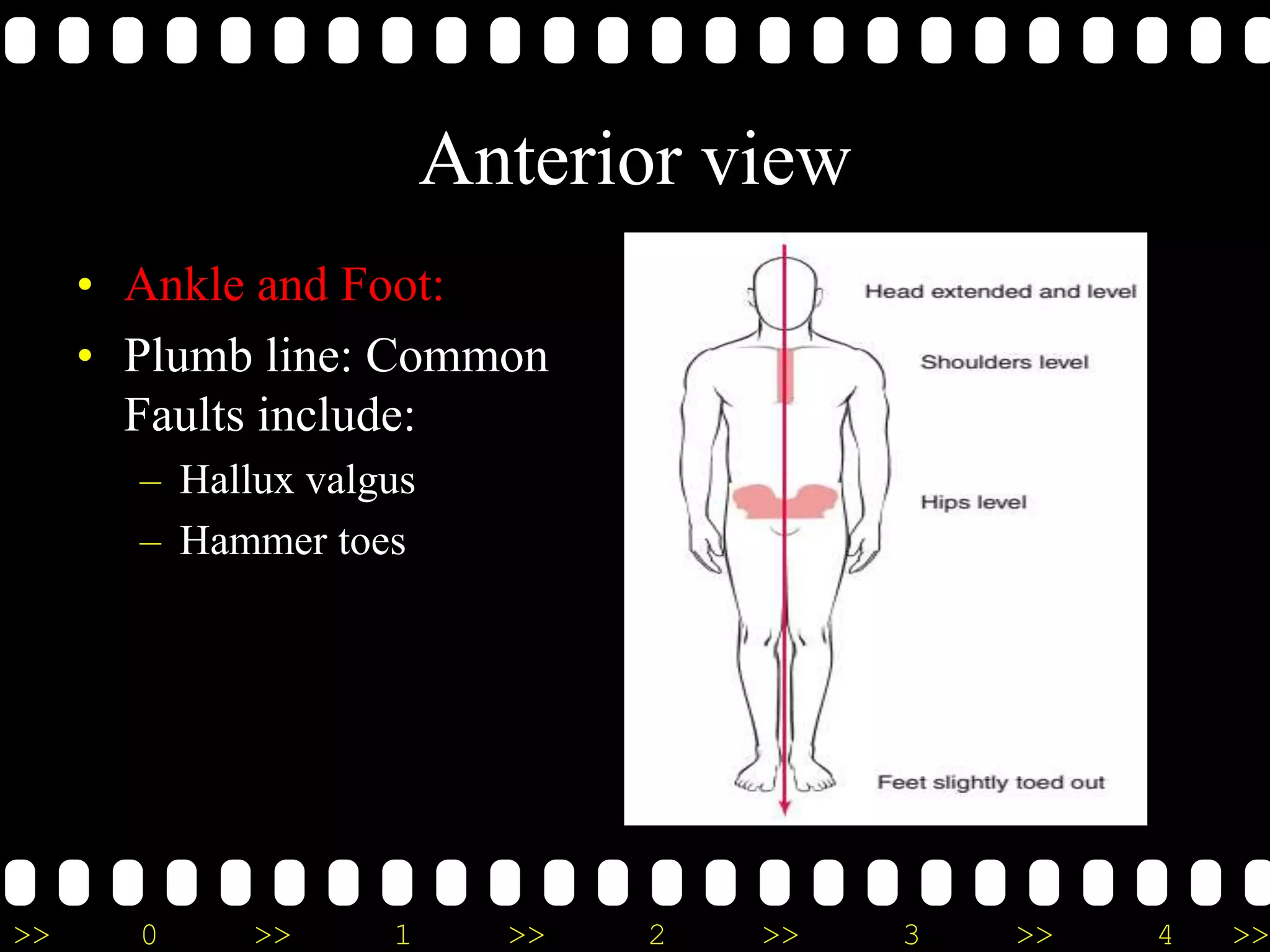
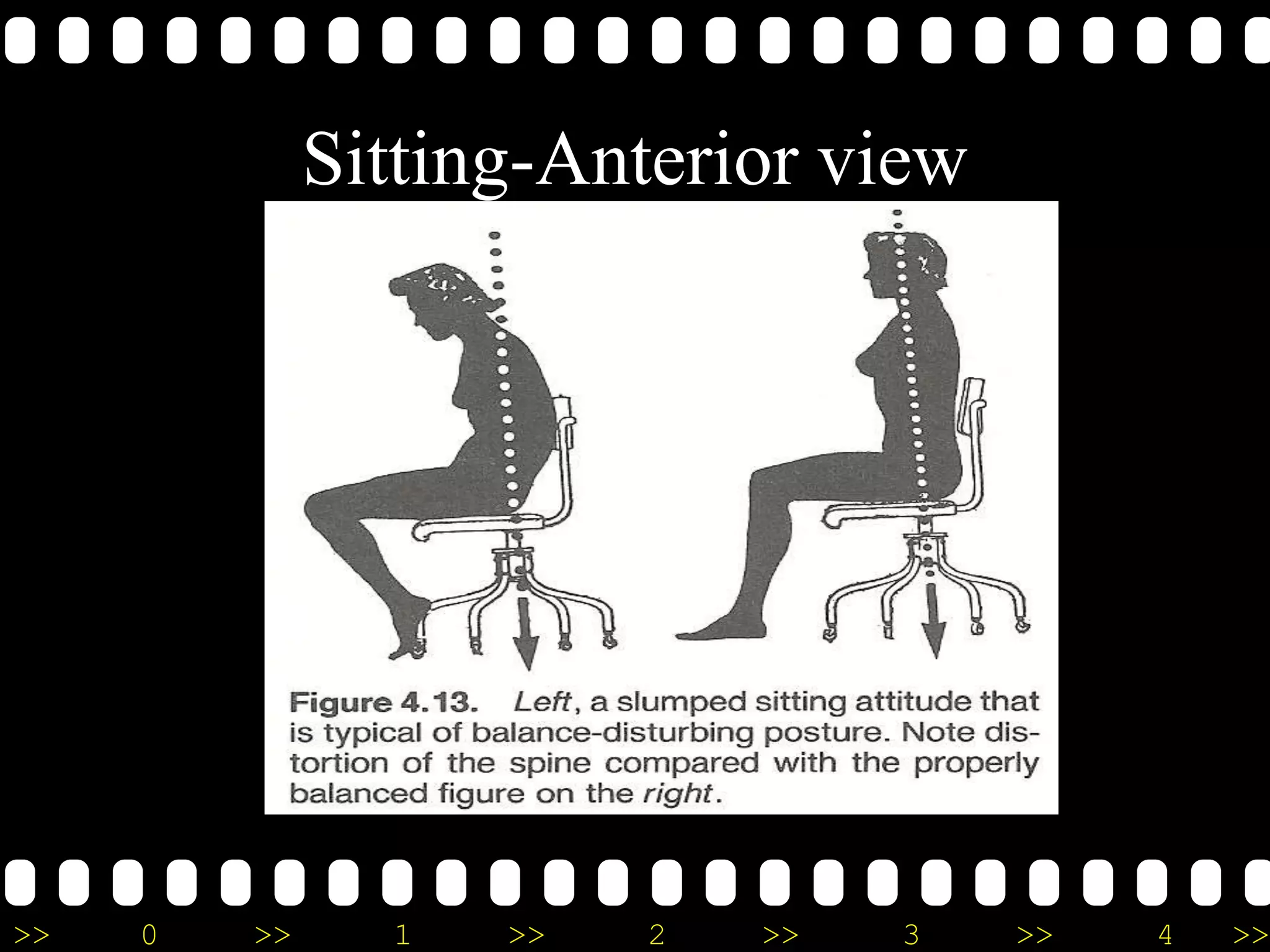
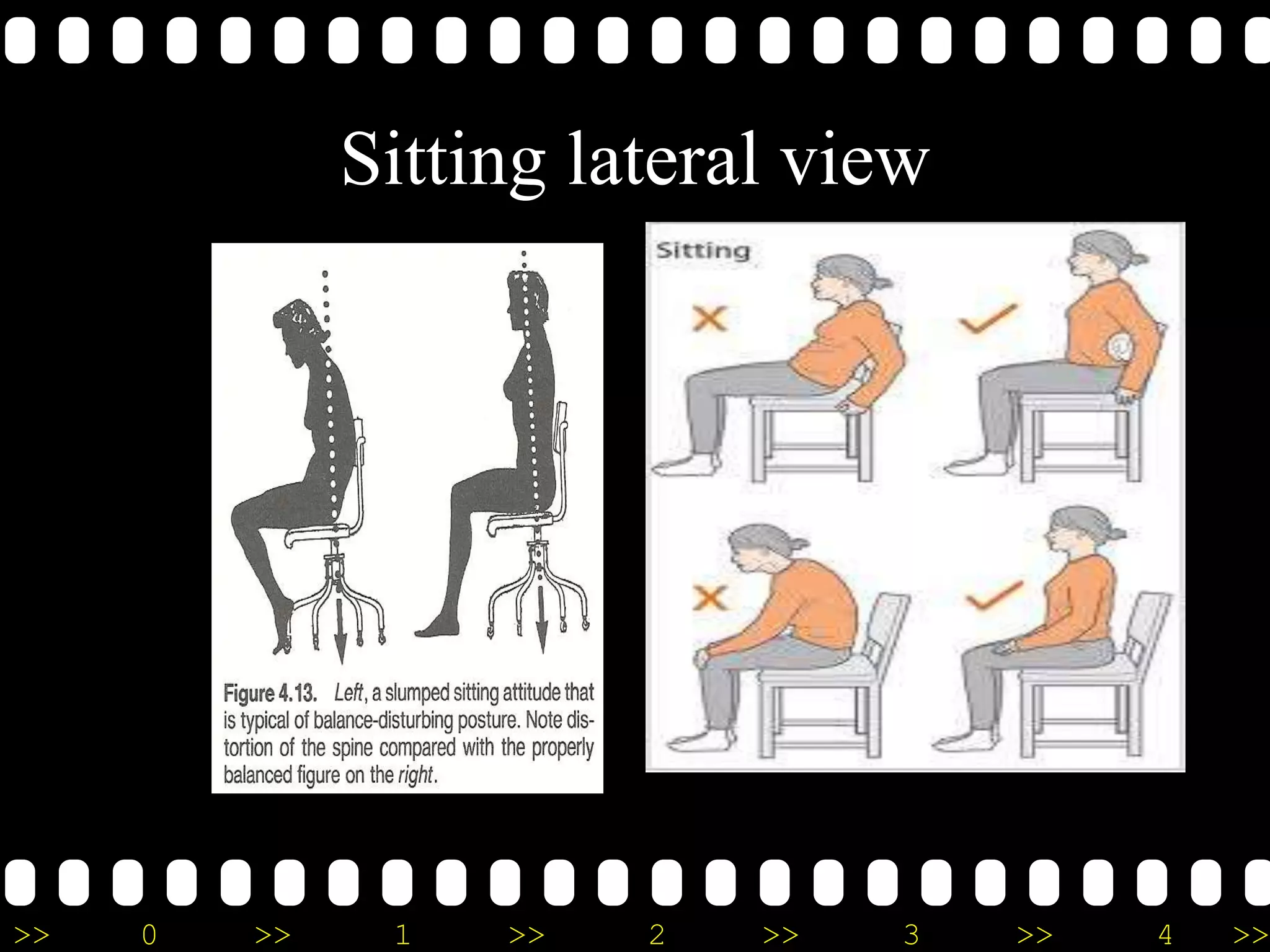

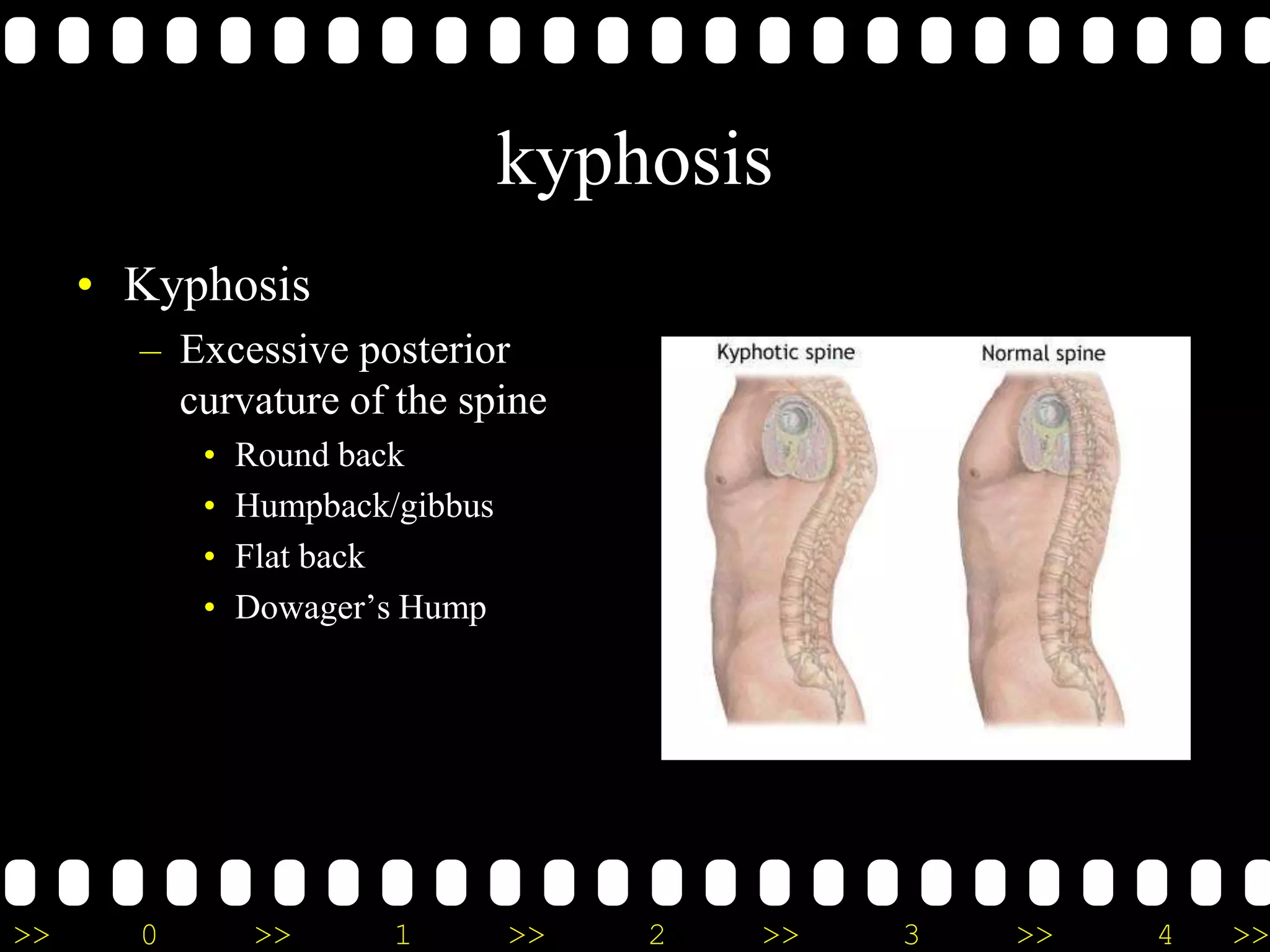
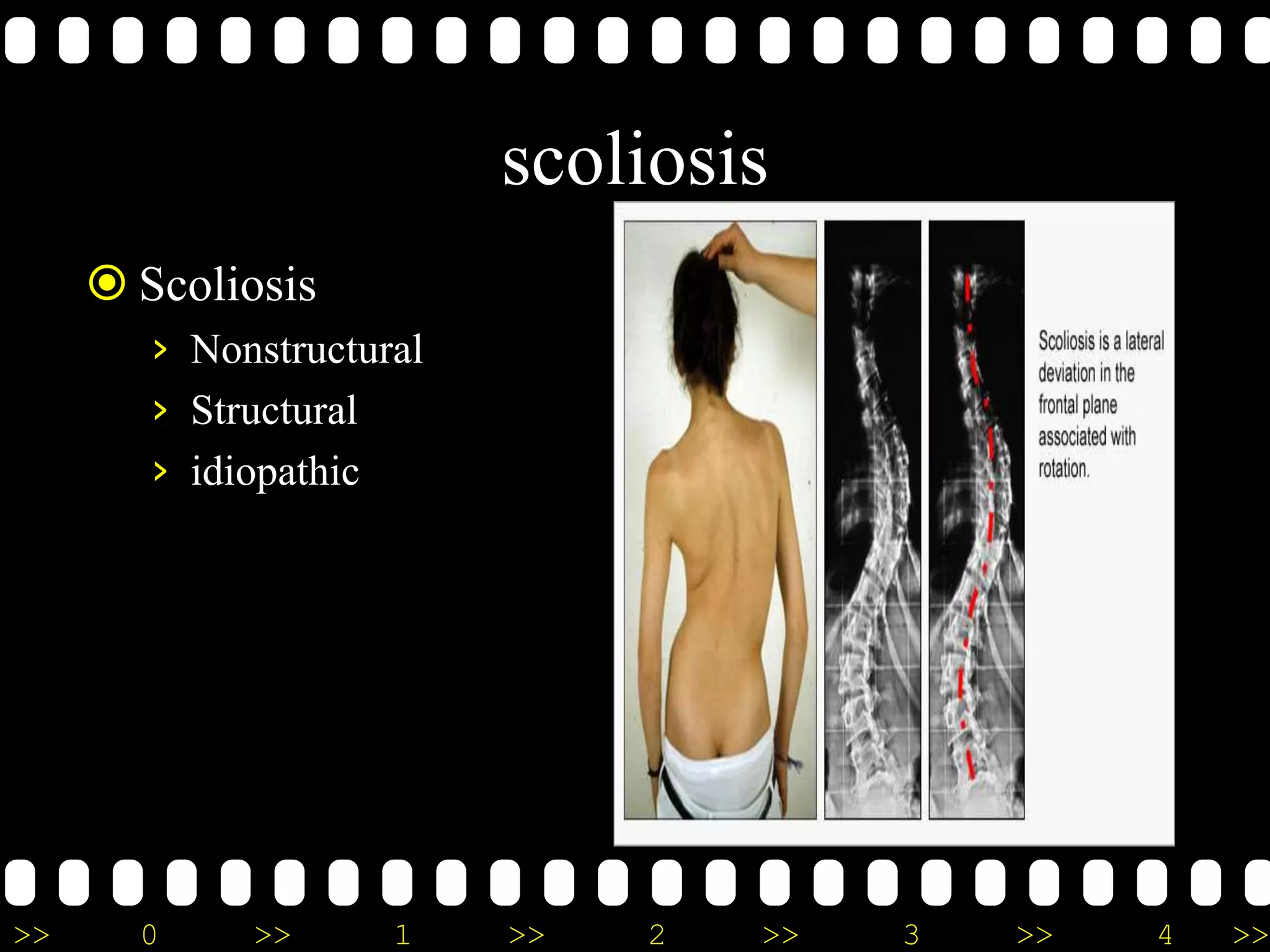
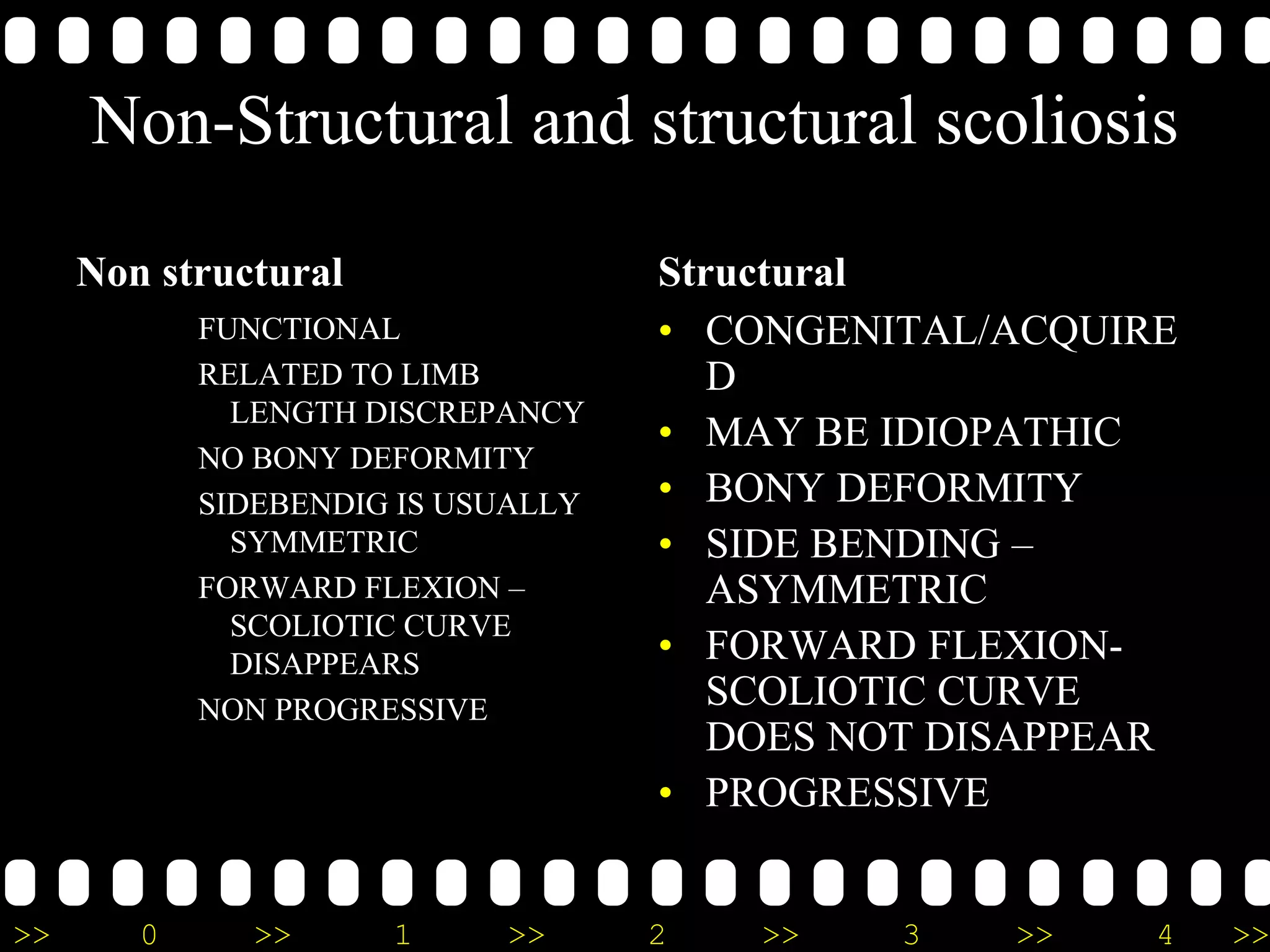


This document provides information on posture assessment, including history taking, observation, and functional testing. Observation involves using a plumb line to evaluate posture from the lateral, anterior, and posterior views in both standing and sitting positions. Common deviations like lordosis, kyphosis, and scoliosis are described. Functional tests evaluate soft tissue and bony restrictions. The goal of assessment is to identify postural deviations and musculoskeletal issues.





















































































