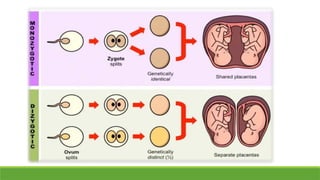
Multiple pregnancies present significant challenges due to increased maternal and fetal complications, influenced by factors such as late childbearing and assisted reproductive techniques. The document details the types, definitions, and risks associated with twin and multiple pregnancies, including the distinctions between dizygotic and monozygotic twins, and emphasizes the need for careful management to mitigate risks. A study conducted in a tertiary care center reported a prevalence of multiple pregnancies at 0.79% among total deliveries, highlighting the increased morbidity and mortality associated compared to singleton pregnancies.